

Inconsistent mammography perceptions and practices among women at risk of breast cancer following a pediatric malignancy: a report from the Childhood Cancer Survivor Study
- PMID: 20506037
- PMCID: PMC2941535
- DOI: 10.1007/s10552-010-9587-5
Inconsistent mammography perceptions and practices among women at risk of breast cancer following a pediatric malignancy: a report from the Childhood Cancer Survivor Study
Abstract
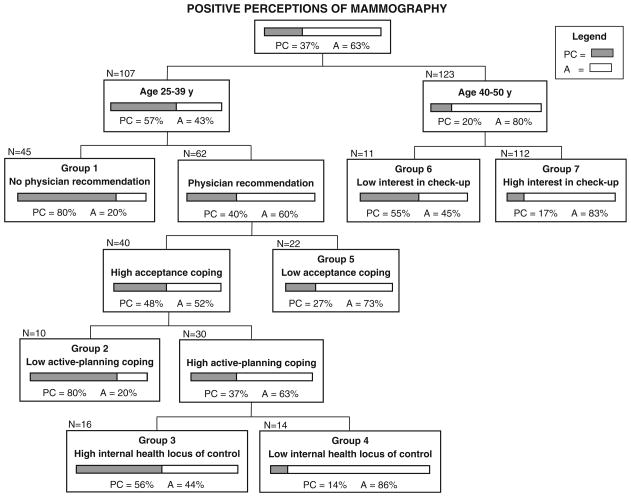
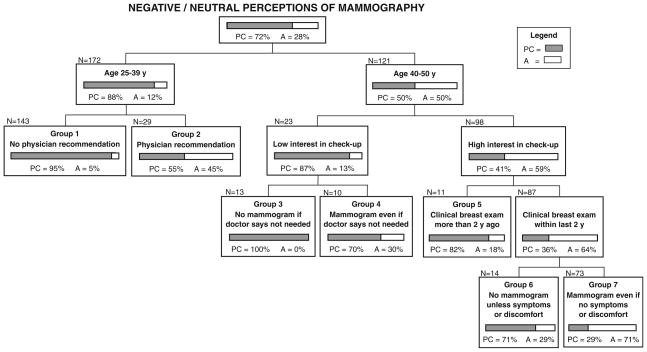
Women treated with chest radiation for a pediatric cancer have low mammography screening rates despite their high risk for breast cancer. This study characterized the relationship between perceptions of mammography and screening practices. A cross-sectional survey was administered to 523 women in North America who were treated with chest radiation before 21 years of age. Women with inconsistent mammography perceptions and practices were identified using the Pros and Cons of Mammography for perceptions and Transtheoretical Model stages of adoption for prior and intended screening practices. Classification and regression tree (CART) analysis was used to identify barriers to and facilitators of screening among women with positive and negative perceptions. Nearly one-third of the cohort had inconsistent perceptions and practices: 37.4% had positive perceptions and were not having mammograms; 27.6% had negative/neutral perceptions and were having mammograms. Regardless of perceptions, a recent physician's recommendation for mammography, age ≥ 40, and interest in routine health care were universally associated with mammography practices. For women with positive perceptions and a physician's recommendation, barriers to screening included high acceptance coping, low active-planning coping, and high internal health locus of control. For women with negative perceptions, acknowledging the importance of asymptomatic screening was associated with mammography.
Figures
References
-
- Bhatia S, Yasui Y, Robison LL, et al. High risk of subsequent neoplasms continues with extended follow-up of childhood Hodgkin’s disease: report from the late effects study group. J Clin Oncol. 2003;21(23):4386–4394. - PubMed
-
- Guibout C, Adjadj E, Rubino C, et al. Malignant breast tumors after radiotherapy for a first cancer during childhood. J Clin Oncol. 2005;23(1):197–204. - PubMed
-
- Kenney LB, Yasui Y, Inskip PD, et al. Breast cancer after childhood cancer: a report from the Childhood Cancer Survivor Study. Ann Intern Med. 2004;141(8):590–597. - PubMed
-
- Metayer C, Lynch CF, Clarke EA, et al. Second cancers among long-term survivors of Hodgkin’s disease diagnosed in childhood and adolescence. J Clin Oncol. 2000;18(12):2435–2443. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
