

Close temporal relationship between onset of cancer and scleroderma in patients with RNA polymerase I/III antibodies
- PMID: 20506513
- PMCID: PMC2946521
- DOI: 10.1002/art.27549
Close temporal relationship between onset of cancer and scleroderma in patients with RNA polymerase I/III antibodies
Abstract
Objective: This study was undertaken to examine the temporal relationship between scleroderma development and malignancy, and to evaluate whether this differs by autoantibody status among affected patients.
Methods: Study participants had a diagnosis of scleroderma, a diagnosis of cancer, cancer, an available serum sample, and a cancer pathology specimen. Sera were tested for autoantibodies against topoisomerase I, centromere, and RNA polymerase I/III by immunoprecipitation and/or enzyme-linked immunosorbent assay. Clinical and demographic characteristics were compared across autoantibody categories. Expression of RNA polymerases I and III was evaluated by immunohistochemistry using cancerous tissue from patients with anti-RNA polymerase antibodies.
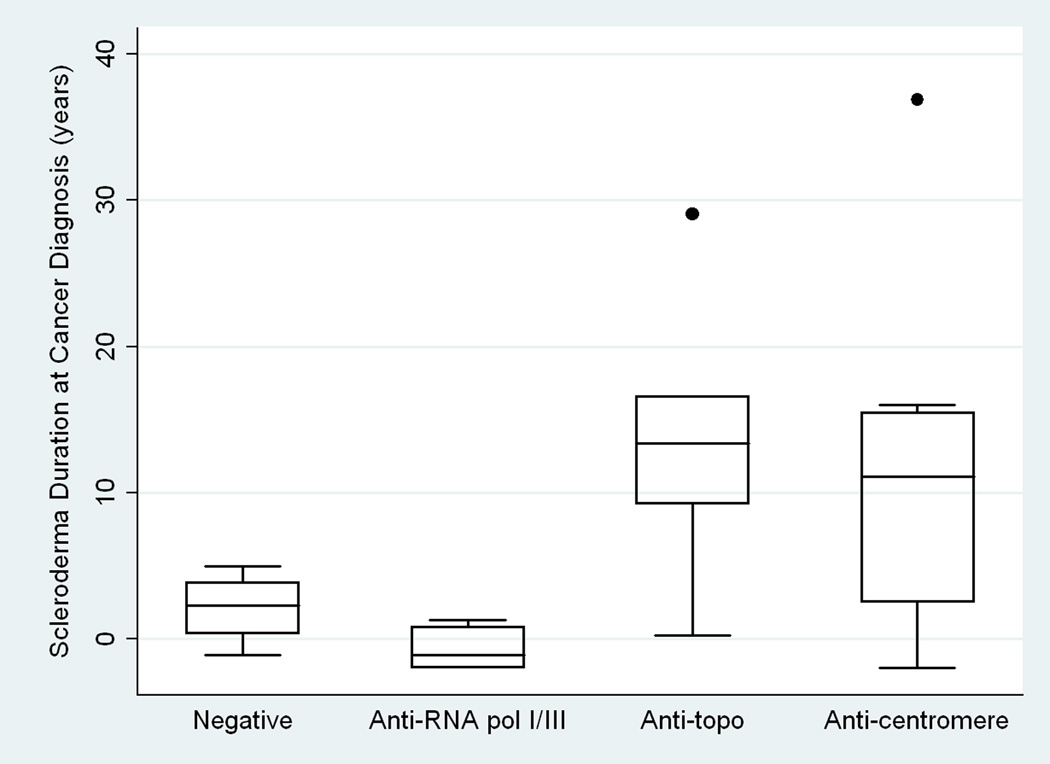
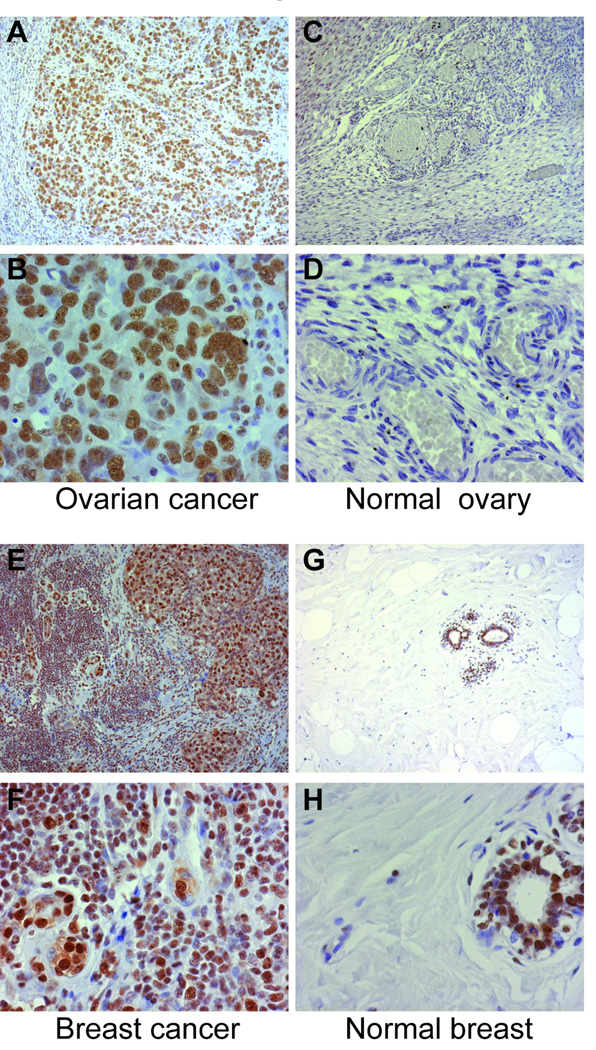
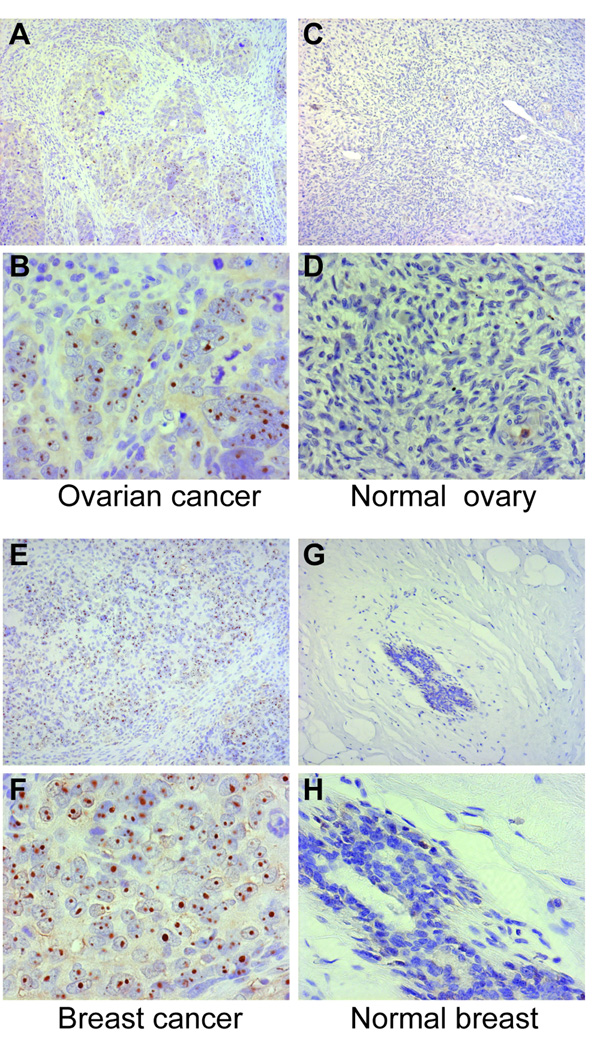
Results: Twenty-three patients were enrolled. Six patients tested positive for anti-RNA polymerase I/III, 5 for anti-topoisomerase I, and 8 for anticentromere, and 4 were not positive for any of these antigens. The median duration of scleroderma at cancer diagnosis differed significantly between groups (-1.2 years in the anti-RNA polymerase I/III group, +13.4 years in the anti-topoisomerase I group, +11.1 years in the anticentromere group, and +2.3 years in the group that was negative for all antigens tested) (P = 0.027). RNA polymerase III demonstrated a robust nucleolar staining pattern in 4 of 5 available tumors from patients with antibodies to RNA polymerase I/III. In contrast, nucleolar RNA polymerase III staining was not detected in any of 4 examined tumors from the RNA polymerase antibody-negative group (P = 0.048).
Conclusion: Our findings indicate that there is a close temporal relationship between the onset of cancer and scleroderma in patients with antibodies to RNA polymerase I/III, which is distinct from scleroderma patients with other autoantibody specificities. In this study, autoantibody response and tumor antigen expression are associated. We propose that malignancy may initiate the scleroderma-specific immune response and drive disease in a subset of scleroderma patients.
Figures
References
-
- Abu-Shakra M, Guillemin F, Lee P. Cancer in systemic sclerosis. Arthritis Rheum. 1993 Apr;36(4):460–464. - PubMed
-
- Derk CT, Rasheed M, Artlett CM, Jimenez SA. A cohort study of cancer incidence in systemic sclerosis. J Rheumatol. 2006 Jun;33(6):1113–1116. - PubMed
-
- Peters-Golden M, Wise RA, Hochberg M, Stevens MB, Wigley FM. Incidence of lung cancer in systemic sclerosis. J Rheumatol. 1985 Dec;12(6):1136–1139. - PubMed
-
- Rosenthal AK, McLaughlin JK, Gridley G, Nyren O. Incidence of cancer among patients with systemic sclerosis. Cancer. 1995 Sep 1;76(5):910–914. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01 AR044684/AR/NIAMS NIH HHS/United States
- P50 HL084946/HL/NHLBI NIH HHS/United States
- R37-DE-12354/DE/NIDCR NIH HHS/United States
- K23 AR052742/AR/NIAMS NIH HHS/United States
- R37 DE012354/DE/NIDCR NIH HHS/United States
- 1K23-AR-052742/AR/NIAMS NIH HHS/United States
- P30-AR-058885/AR/NIAMS NIH HHS/United States
- R01-AR-044684/AR/NIAMS NIH HHS/United States
- P30-AR-053503/AR/NIAMS NIH HHS/United States
- T32 AR048522/AR/NIAMS NIH HHS/United States
- P30 AR058885/AR/NIAMS NIH HHS/United States
- P30 AR053503/AR/NIAMS NIH HHS/United States
- 1P50-HL-084946-01/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
