

Clinical characteristics and outcomes of sepsis-related vs non-sepsis-related ARDS
- PMID: 20507948
- PMCID: PMC2940067
- DOI: 10.1378/chest.09-2933
Clinical characteristics and outcomes of sepsis-related vs non-sepsis-related ARDS
Abstract
Background: ARDS may occur after either septic or nonseptic injuries. Sepsis is the major cause of ARDS, but little is known about the differences between sepsis-related and non-sepsis-related ARDS.
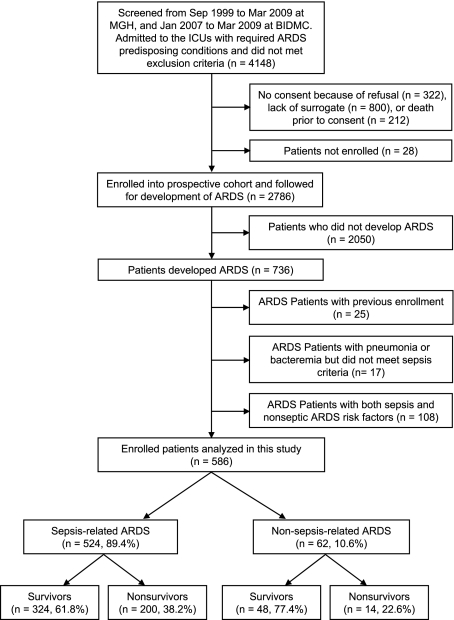
Methods: A total of 2,786 patients with ARDS-predisposing conditions were enrolled consecutively into a prospective cohort, of which 736 patients developed ARDS. We defined sepsis-related ARDS as ARDS developing in patients with sepsis and non-sepsis-related ARDS as ARDS developing after nonseptic injuries, such as trauma, aspiration, and multiple transfusions. Patients with both septic and nonseptic risks were excluded from analysis.
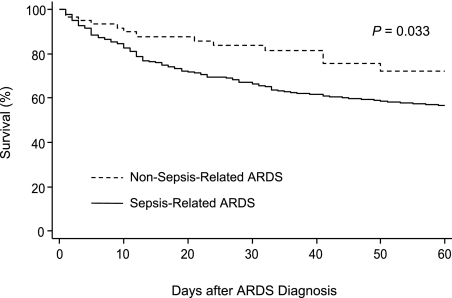
Results: Compared with patients with non-sepsis-related ARDS (n = 62), patients with sepsis-related ARDS (n = 524) were more likely to be women and to have diabetes, less likely to have preceding surgery, and had longer pre-ICU hospital stays and higher APACHE III (Acute Physiology and Chronic Health Evaluation III) scores (median, 78 vs 65, P < .0001). There were no differences in lung injury score, blood pH, Pao(2)/Fio(2) ratio, and Paco(2) on ARDS diagnosis. However, patients with sepsis-related ARDS had significantly lower Pao(2)/Fio(2) ratios than patients with non-sepsis-related ARDS patients on ARDS day 3 (P = .018), day 7 (P = .004), and day 14 (P = .004) (repeated-measures analysis, P = .011). Compared with patients with non-sepsis-related ARDS, those with sepsis-related had a higher 60-day mortality (38.2% vs 22.6%; P = .016), a lower successful extubation rate (53.6% vs 72.6%; P = .005), and fewer ICU-free days (P = .0001) and ventilator-free days (P = .003). In multivariate analysis, age, APACHE III score, liver cirrhosis, metastatic cancer, admission serum bilirubin and glucose levels, and treatment with activated protein C were independently associated with 60-day ARDS mortality. After adjustment, sepsis-related ARDS was no longer associated with higher 60-day mortality (hazard ratio, 1.26; 95% CI, 0.71-2.22).
Conclusion: Sepsis-related ARDS has a higher overall disease severity, poorer recovery from lung injury, lower successful extubation rate, and higher mortality than non-sepsis-related ARDS. Worse clinical outcomes in sepsis-related ARDS appear to be driven by disease severity and comorbidities.
Figures
References
-
- Phua J, Badia JR, Adhikari NK, et al. Has mortality from acute respiratory distress syndrome decreased over time? A systematic review. Am J Respir Crit Care Med. 2009;179(3):220–227. - PubMed
-
- Wheeler AP, Bernard GR. Acute lung injury and the acute respiratory distress syndrome: a clinical review. Lancet. 2007;369(9572):1553–1564. - PubMed
-
- Ware LB, Matthay MA. The acute respiratory distress syndrome. N Engl J Med. 2000;342(18):1334–1349. - PubMed
-
- Matthay MA, Zimmerman GA, Esmon C, et al. Future research directions in acute lung injury: summary of a National Heart, Lung, and Blood Institute working group. Am J Respir Crit Care Med. 2003;167(7):1027–1035. - PubMed
-
- Hudson LD, Steinberg KP. Epidemiology of acute lung injury and ARDS. Chest. 1999;116(1) Suppl:74S–82S. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
