

Dry-weight: a concept revisited in an effort to avoid medication-directed approaches for blood pressure control in hemodialysis patients
- PMID: 20507951
- PMCID: PMC2893058
- DOI: 10.2215/CJN.01760210
Dry-weight: a concept revisited in an effort to avoid medication-directed approaches for blood pressure control in hemodialysis patients
Abstract
Background and objectives: Achieving and maintaining dry-weight appears to be an effective but forgotten strategy in controlling and maintaining normotension among hypertensive patients on hemodialysis.
Methods: Qualitative review of literature to define dry-weight and its utility in achieving blood pressure control.
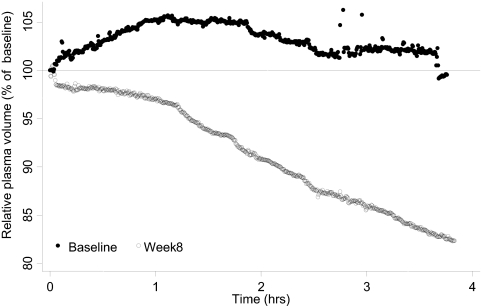
Results: The concept of dry-weight has evolved over time and its definition has changed. One such definition defines dry-weight as the lowest tolerated postdialysis weight achieved via gradual change in postdialysis weight at which there are minimal signs or symptoms of hypovolemia or hypervolemia. Although clinical examination does not perform well in detecting latent increase in dry-weight, several technologies such as relative plasma volume monitoring and body impedance analysis are emerging that may help in assessing dry-weight in the future. Sodium restriction is a modifiable risk factor that can lead to better blood pressure (BP) control. However, dietary sodium restriction requires lifestyle modifications that are difficult to implement and even harder to sustain over the long term. Restricting dialysate sodium is a simpler but underexplored strategy that can reduce thirst, limit interdialytic weight gain, and assist the achievement of dry-weight. Achievement of dry-weight can improve interdialytic BP, reduce pulse pressure, and limit hospitalizations.
Conclusions: Avoiding medication-directed control of BP may enhance the opportunity to probe dry-weight, facilitate removal of volume, and limit the risk for pressure-volume overload, which may be a significant concern leading to myocardial remodeling in the hemodialysis patient. Probing dry-weight among patients with ESRD has the potential to improve dismal cardiovascular outcomes.
Figures
References
-
- Lazarus JM, Hampers C, Merrill JP: Hypertension in chronic renal failure. Treatment with hemodialysis and nephrectomy. Arch Intern Med 133: 1059–1066, 1974 - PubMed
-
- Kalantar-Zadeh K, Block G, Humphreys MH, Kopple JD: Reverse epidemiology of cardiovascular risk factors in maintenance dialysis patients. Kidney Int 63: 793–808, 2003 - PubMed
-
- Foley RN, Agarwal R: Hypertension is harmful to dialysis patients and should be controlled. Semin Dial 20: 518–522, 2007 - PubMed
-
- Li Z, Lacson E, Jr, Lowrie EG, Ofsthun NJ, Kuhlmann MK, Lazarus JM, Levin NW: The epidemiology of systolic blood pressure and death risk in hemodialysis patients. Am J Kidney Dis 48: 606–615, 2006 - PubMed
-
- Heerspink HJ, Ninomiya T, Zoungas S, de ZD, Grobbee DE, Jardine MJ, Gallagher M, Roberts MA, Cass A, Neal B, Perkovic V: Effect of lowering blood pressure on cardiovascular events and mortality in patients on dialysis: A systematic review and meta-analysis of randomised controlled trials. Lancet 373: 1009–1015, 2009 - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
