

Contemporary management of fibroids in pregnancy
Rev Obstet Gynecol.
2010 Winter.
Abstract
Uterine fibroids are a very common finding in women of reproductive age. The majority of fibroids do not change their size during pregnancy, but one-third may grow in the first trimester. Although the data are conflicting and most women with fibroids have uneventful pregnancies, the weight of evidence in the literature suggests that uterine fibroids are associated with an increased rate of spontaneous miscarriage, preterm labor, placenta abruption, malpresentation, labor dystocia, cesarean delivery, and postpartum hemorrhage.
Keywords: Fetal anomalies; Fibroids; Miscarriage; Myomectomy; Placenta abruption; Preterm labor; Uterine artery embolization.
Figures
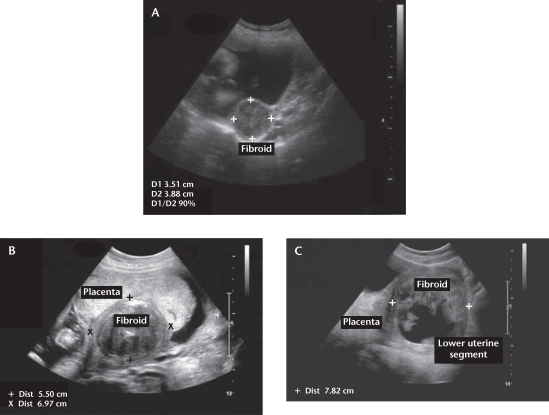
Representative images of fibroids in pregnancy. (A) A 3.5 × 3.8 cm fibroid is evident in the posterior uterine wall. This small fibroid is unlikely to cause any pregnancy-related complications. (B) A 5.5 × 6.9 cm retroplacental fibroid is shown. This large fibroid is likely to interfere with placentation and uteroplacental blood flow due both to its size and location, which may present clinically as intrauterine growth restriction, placental abruption, or preeclampsia. (C) A 7.8 cm fibroid is evident in the lower uterine segment. Given its size and location, this large fibroid may interfere with engagement of the fetal head near term and the normal progress of labor. Moreover, the internal echogenic changes are consistent with “red degeneration,” and would likely account for the patient’s lower abdominal pain.
References
-
- Day Baird D, Dunson DB, Hill MC, et al. High cumulative incidence of uterine leiomyoma in black and white women: ultrasound evidence. Am J Obstet Gynecol. 2003;188:100–107. - PubMed
-
- Muram D, Gillieson M, Walters JH. Myomas of the uterus in pregnancy: ultrasonographic follow-up. Am J Obstet Gynecol. 1980;138:16–19. - PubMed
-
- Burton CA, Grimes DA, March CM. Surgical management of leiomyomata during pregnancy. Obstet Gynecol. 1989;74:707–709. - PubMed
-
- Rice JP, Kay HH, Mahony BS. The clinical significance of uterine leiomyomas in pregnancy. Am J Obstet Gynecol. 1989;160:1212–1216. - PubMed
-
- Qidwai GI, Caughey AB, Jacoby AF. Obstetric outcomes in women with sonographically identified uterine leiomyomata. Obstet Gynecol. 2006;107:376–382. - PubMed
LinkOut - more resources
Full Text Sources