

Pathobiological features of small hepatocellular carcinoma: correlation between tumor size and biological behavior
- PMID: 20508947
- PMCID: PMC11827968
- DOI: 10.1007/s00432-010-0909-5
Pathobiological features of small hepatocellular carcinoma: correlation between tumor size and biological behavior
Abstract
Purpose: Increasing evidence has suggested that tumor size is one of the independent prognostic factors of patients with hepatocellular carcinoma (HCC). However, the criteria used to determine when HCC should be classified as small remain controversial. Our objective was to evaluate the relationship between the size of HCC and its clinicopathological features.
Methods: A retrospective study on 618 patients who underwent partial hepatectomy for solitary HCC was performed. These patients were divided into Groups 1-5 according to the tumor diameter: ≤ 1, 1.1-2, 2.1-3, 3.1-5 and >5 cm, respectively. The clinicopathological variables of the patients in each group were compared statistically.
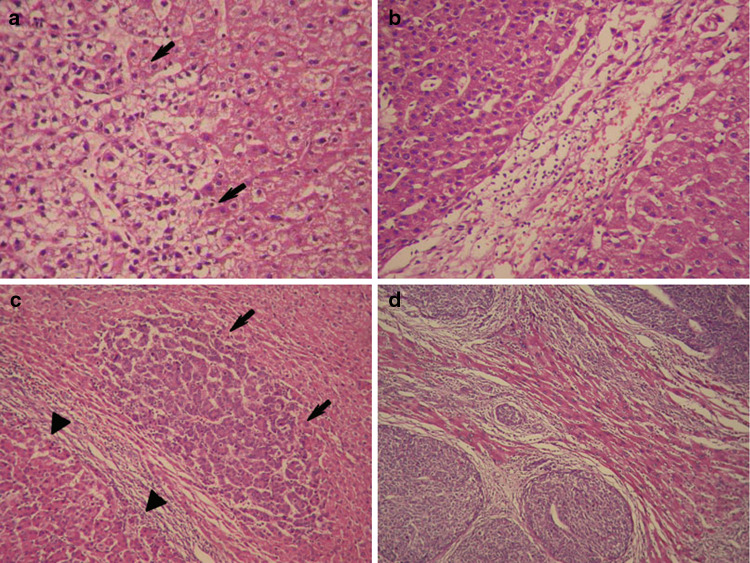
Results: Except for the microHCC (≤ 1 cm) which differed significantly from the other four groups in the clinicopathological variables, almost no differences existed among HCC ranging from 1 to 3 cm, or HCCs > 3 cm. If ≤ 3 cm was used as the cut-off point for small HCC (SHCC), and >3 cm for large HCC (LHCC), significant differences (P < 0.05-0.01) were observed between SHCC and LHCC in: histological grades I-II (48.0 vs. 19.4 %), capsular invasion (15.4 vs. 36.3%), tumor thrombi (6.9 vs. 23.5%), satellite nodules (12.3 vs. 35.5%), noninvasive growth patterns (69.6 vs. 25.4%), the overall survival (OS, 119.6 ± 34.7 vs. 68.5 ± 6.6 months), and the recurrence-free survival (RFS, 67.0 ± 16.7 vs. 29.5 ± 3.2 months). Multivariate Cox regression analyses show that tumor size >3 cm was one of the independent prognostic factors for both OS and RFS.
Conclusions: The 3 cm cutoff seems to best determine the biological behavior and clinical prognosis of patients undergoing partial hepatectomy for early stage HCC. Overall, HCC smaller than 3 cm in diameter was closely related with a better prognosis which reflected the relatively benign pathobiological features at an early developmental stage. As HCC > 3 cm exhibited a tendency towards more aggressive behavior, we suggest that HCC ≤ 3 cm in diameter should be used as a critical size of SHCC at which curative treatment achieves better long-term survivals.
Figures


Similar articles
-
[Comparison of the efficacy of anatomical resection versus hepatic parenchymal preservation preference in patients with solitary small hepatocellular carcinoma and cirrhosis: a multicenter retrospective study].Zhonghua Gan Zang Bing Za Zhi. 2025 Apr 20;33(4):348-358. doi: 10.3760/cma.j.cn501113-20250315-00097. Zhonghua Gan Zang Bing Za Zhi. 2025. PMID: 40419370 Chinese.
-
Percutaneous ethanol injection or percutaneous acetic acid injection for early hepatocellular carcinoma.Cochrane Database Syst Rev. 2015 Jan 26;1(1):CD006745. doi: 10.1002/14651858.CD006745.pub3. Cochrane Database Syst Rev. 2015. PMID: 25620061 Free PMC article.
-
Impact of residual disease as a prognostic factor for survival in women with advanced epithelial ovarian cancer after primary surgery.Cochrane Database Syst Rev. 2022 Sep 26;9(9):CD015048. doi: 10.1002/14651858.CD015048.pub2. Cochrane Database Syst Rev. 2022. PMID: 36161421 Free PMC article.
-
A randomized controlled trial of hepatectomy with adjuvant transcatheter arterial chemoembolization versus hepatectomy alone for Stage III A hepatocellular carcinoma.J Cancer Res Clin Oncol. 2009 Oct;135(10):1437-45. doi: 10.1007/s00432-009-0588-2. Epub 2009 May 1. J Cancer Res Clin Oncol. 2009. PMID: 19408012 Free PMC article. Clinical Trial.
-
Optimal primary surgical treatment for advanced epithelial ovarian cancer.Cochrane Database Syst Rev. 2011 Aug 10;2011(8):CD007565. doi: 10.1002/14651858.CD007565.pub2. Cochrane Database Syst Rev. 2011. PMID: 21833960 Free PMC article.
Cited by
-
Small hepatocellular carcinoma: current and future approaches.Hepatol Int. 2013 Jul;7(3):805-12. doi: 10.1007/s12072-013-9454-z. Epub 2013 Aug 6. Hepatol Int. 2013. PMID: 26201917
-
Prognostic value of preoperative computed tomography in HBV-related hepatocellular carcinoma patients after curative resection.Onco Targets Ther. 2019 May 16;12:3791-3804. doi: 10.2147/OTT.S199136. eCollection 2019. Onco Targets Ther. 2019. PMID: 31190879 Free PMC article.
-
Preoperative Prediction of Microvascular Invasion in Patients With Hepatocellular Carcinoma Based on Radiomics Nomogram Using Contrast-Enhanced Ultrasound.Front Oncol. 2021 Sep 7;11:709339. doi: 10.3389/fonc.2021.709339. eCollection 2021. Front Oncol. 2021. PMID: 34557410 Free PMC article.
-
Prognostic factors affecting postoperative survival of patients with solitary small hepatocellular carcinoma.Chin J Cancer. 2016 Aug 16;35(1):80. doi: 10.1186/s40880-016-0143-x. Chin J Cancer. 2016. PMID: 27527497 Free PMC article.
-
Clinical and laboratory parameters associated with li-rads as diagnostic of liver nodule in patients with cirrhosis.Transl Gastroenterol Hepatol. 2021 Oct 25;6:55. doi: 10.21037/tgh.2020.01.05. eCollection 2021. Transl Gastroenterol Hepatol. 2021. PMID: 34805577 Free PMC article.
References
-
- Aishima S, Nishihara Y, Kuroda Y, Taguchi K, Iguchi T, Taketomi A et al (2007) Histologic characteristics and prognostic significance in small hepatocellular carcinoma with biliary differentiation: subdivision and comparison with ordinary hepatocellular carcinoma. Am J Surg Pathol 31:783–791 - PubMed
-
- Arii S, Yamaoka Y, Futagawa S, Inoue K, Kobayashi K, Kojiro M et al (2000) Results of surgical and nonsurgical treatment for small-sized hepatocellular carcinomas: a retrospective and nationwide survey in Japan. The Liver Cancer Study Group of Japan. Hepatology 32:1224–1229 - PubMed
-
- Chung H, Kudo M, Takahashi S, Hagiwara S, Sakaguchi Y, Inoue T et al (2008) Comparison of three current staging systems for hepatocellular carcinoma: Japan integrated staging score, new Barcelona Clinic Liver Cancer staging classification, and Tokyo score. J Gastroenterol Hepatol 23:445–452 - PubMed
-
- Cong WM, Wu MC (1990) The biopathologic characteristics of DNA content of hepatocellular carcinomas. Cancer 66:498–501 - PubMed
-
- Cong WM, Wu MC, Zhang XZ (1992) Characteristic changes of DNA stemlines during hepatocarcinogenesis in rats. Chin Med J 105:535–538 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
