

Anatomic and pathologic variability during radiotherapy for a hybrid active breath-hold gating technique
- PMID: 20510201
- PMCID: PMC2956181
- DOI: 10.1016/j.ijrobp.2009.09.080
Anatomic and pathologic variability during radiotherapy for a hybrid active breath-hold gating technique
Abstract
Purpose: To evaluate intra- and interfraction variability of tumor and lung volume and position using a hybrid active breath-hold gating technique.
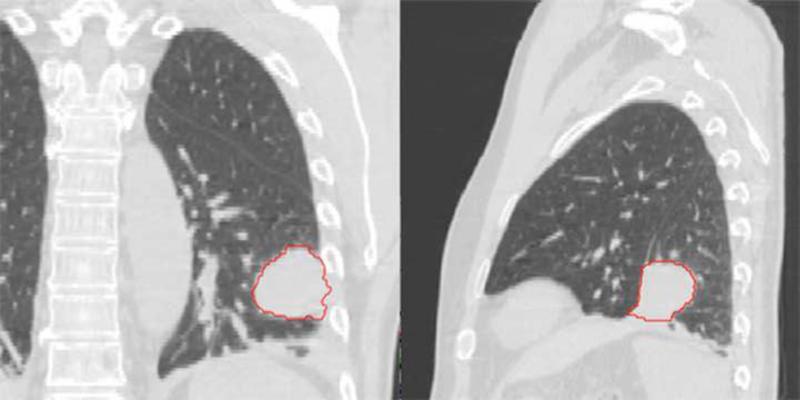
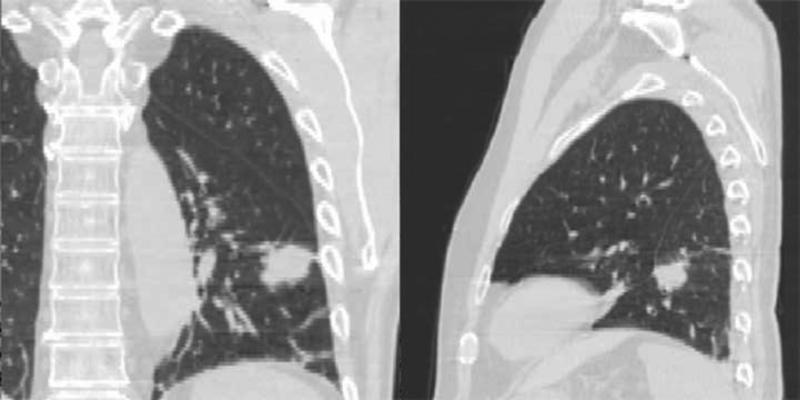
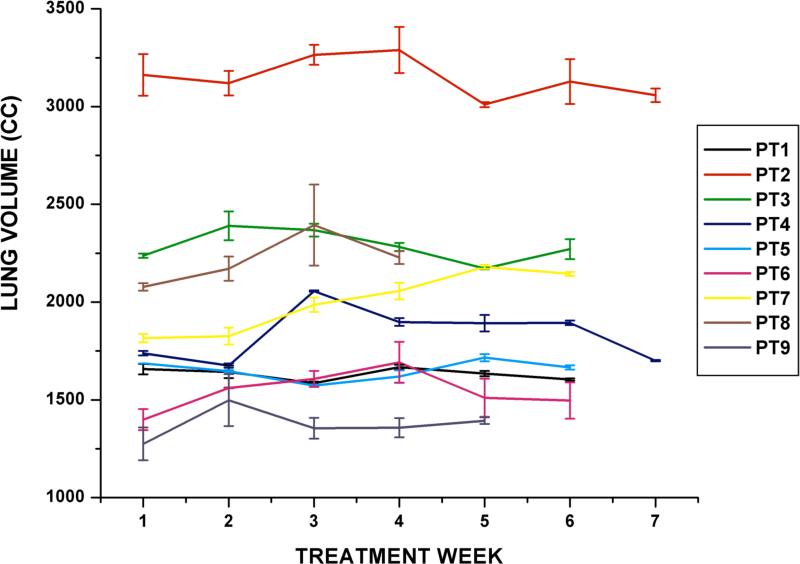
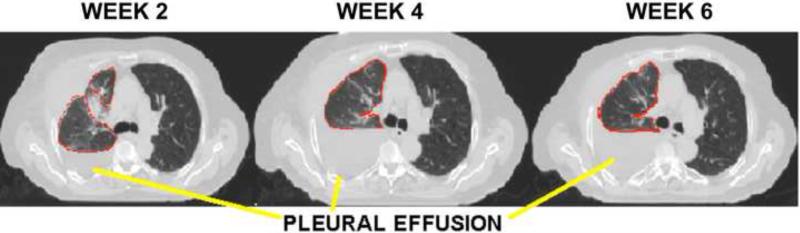
Methods and materials: A total of 159 repeat normal inspiration active breath-hold CTs were acquired weekly during radiotherapy for 9 lung cancer patients (12-21 scans per patient). A physician delineated the gross tumor volume (GTV), lungs, and spinal cord on the first breath-hold CT, and contours were propagated semiautomatically. Intra- and interfraction variability of tumor and lung position and volume were evaluated. Tumor centroid and border variability were quantified.
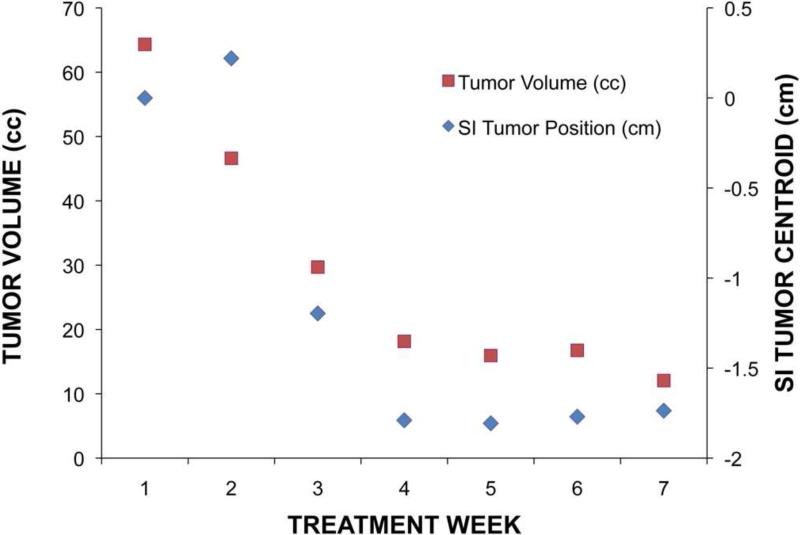
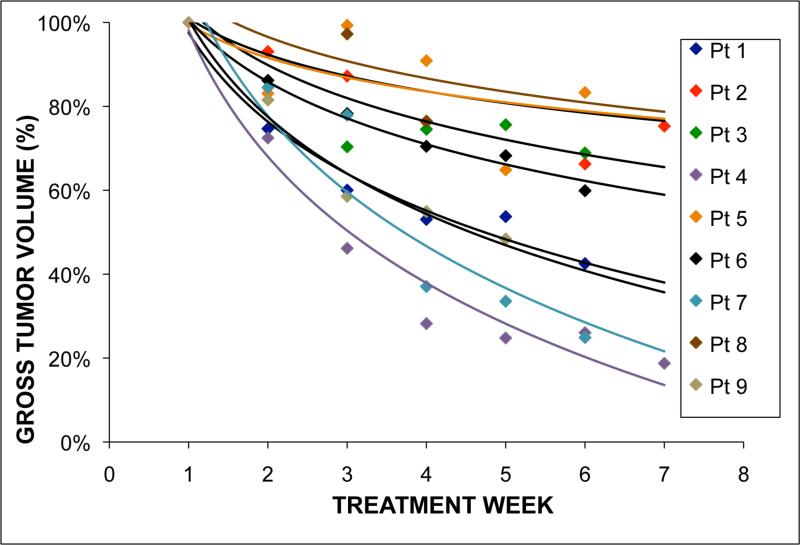
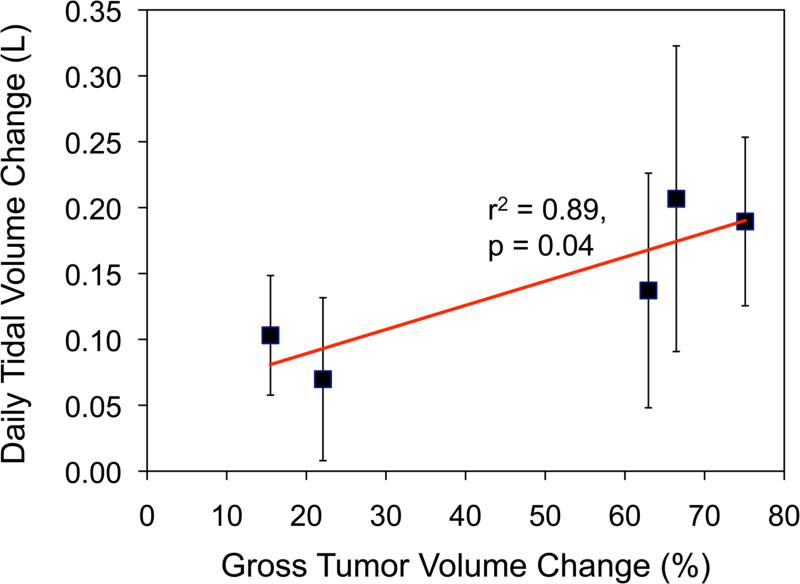
Results: On average, intrafraction variability of lung and GTV centroid position was <2.0 mm. Interfraction population variability was 3.6-6.7 mm (systematic) and 3.1-3.9 mm (random) for the GTV centroid and 1.0-3.3 mm (systematic) and 1.5-2.6 mm (random) for the lungs. Tumor volume regressed 44.6% +/- 23.2%. Gross tumor volume border variability was patient specific and demonstrated anisotropic shape change in some subjects. Interfraction GTV positional variability was associated with tumor volume regression and contralateral lung volume (p < 0.05). Inter-breath-hold reproducibility was unaffected by time point in the treatment course (p > 0.1). Increases in free-breathing tidal volume were associated with increases in breath-hold ipsilateral lung volume (p < 0.05).
Conclusions: The breath-hold technique was reproducible within 2 mm during each fraction. Interfraction variability of GTV position and shape was substantial because of tumor volume and breath-hold lung volume change during therapy. These results support the feasibility of a hybrid breath-hold gating technique and suggest that online image guidance would be beneficial.
(c) 2010 Elsevier Inc. All rights reserved.
Figures
References
-
- Britton KR, Starkschall G, Tucker SL, et al. Assessment of gross tumor volume regression and motion changes during radiotherapy for non-small-cell lung cancer as measured by four-dimensional computed tomography. Int J Radiat Oncol Biol Phys. 2007;68:1036–1046. - PubMed
-
- Hugo G, Vargas C, Liang J, et al. Changes in the respiratory pattern during radiotherapy for cancer in the lung. Radiother Oncol. 2006;78:326–331. - PubMed
-
- Juhler Nottrup T, Korreman SS, Pedersen AN, et al. Intra- and interfraction breathing variations during curative radiotherapy for lung cancer. Radiother Oncol. 2007;84:40–48. - PubMed
-
- Liu HH, Balter P, Tutt T, et al. Assessing respiration-induced tumor motion and internal target volume using four-dimensional computed tomography for radiotherapy of lung cancer. Int J Radiat Oncol Biol Phys. 2007;68:531–540. - PubMed
-
- Mageras GS, Pevsner A, Yorke ED, et al. Measurement of lung tumor motion using respiration-correlated CT. Int J Radiat Oncol Biol Phys. 2004;60:933–941. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
