

Cardiac magnetic resonance with edema imaging identifies myocardium at risk and predicts worse outcome in patients with non-ST-segment elevation acute coronary syndrome
- PMID: 20510215
- PMCID: PMC3675879
- DOI: 10.1016/j.jacc.2010.01.047
Cardiac magnetic resonance with edema imaging identifies myocardium at risk and predicts worse outcome in patients with non-ST-segment elevation acute coronary syndrome
Abstract
Objectives: The aim of this study was to define the prevalence and significance of myocardial edema in patients with non-ST-segment elevation acute coronary syndrome (NSTE-ACS).
Background: Most patients with NSTE-ACS undergo angiography, yet not all have obstructive coronary artery disease (CAD) requiring revascularization. Identifying patients with myocardium at risk could enhance the effectiveness of an early invasive strategy. Cardiac magnetic resonance (CMR) can demonstrate edematous myocardium subjected to ischemia but has not been used to evaluate NSTE-ACS patients.
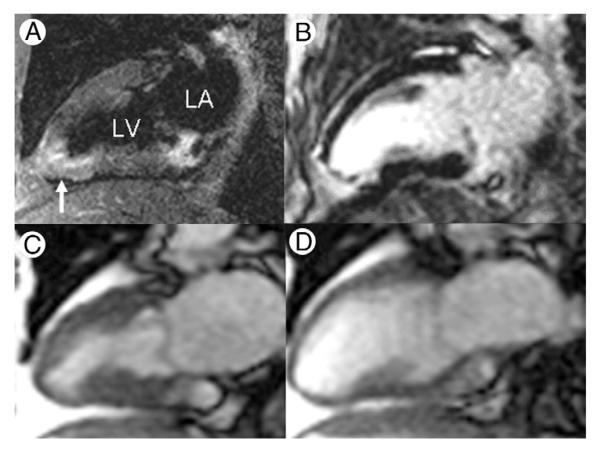
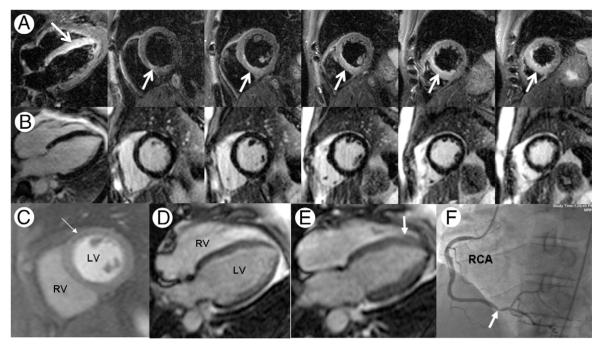
Methods: One hundred consecutive patients with NSTE-ACS were prospectively enrolled to undergo 30-min CMR, including T2-weighted edema imaging and late gadolinium enhancement before coronary angiography. Clinical management including revascularization decision-making was performed without CMR results.
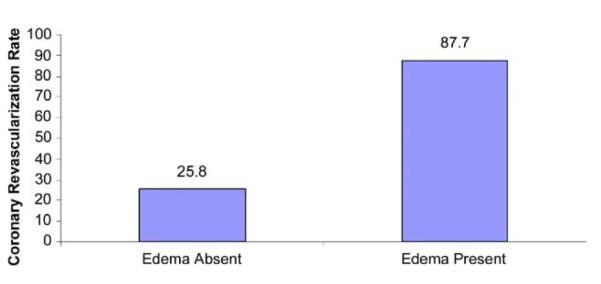
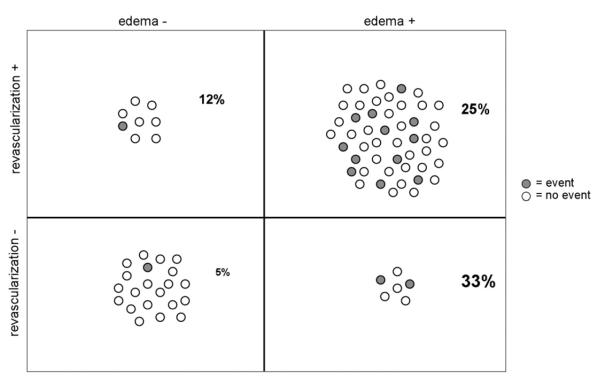
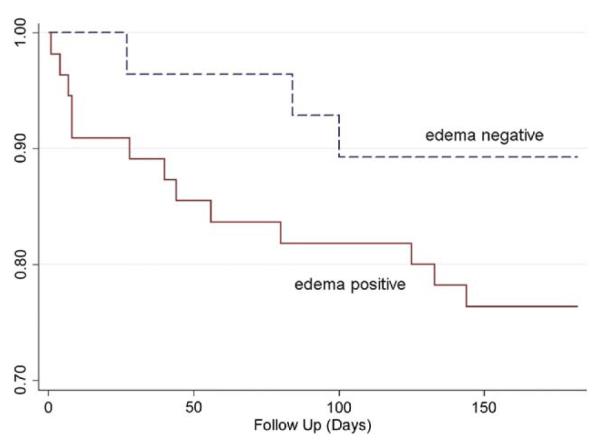
Results: Of 88 adequate CMR studies, 57 (64.8%) showed myocardial edema. Obstructive CAD requiring revascularization was present in 87.7% of edema-positive patients versus 25.8% of edema-negative patients (p < 0.001). By multiple logistic regression analysis after adjusting for late gadolinium enhancement, perfusion, and wall motion scores, TIMI risk score was not predictive of obstructive CAD. Conversely, an increase in T2 score by 1 U increased the odds of subsequent coronary revascularization by 5.70 times (95% confidence interval: 2.38 to 13.62, p < 0.001). Adjusting for peak troponin-I, patients with edema showed a higher hazard of a cardiovascular event or death within 6 months after NSTE-ACS compared with those without edema (hazard ratio: 4.47, 95% confidence interval: 1.00 to 20.03; p = 0.050).
Conclusions: In NSTE-ACS patients, rapid CMR identifies reversibly injured myocardium due to obstructive CAD and predicts worse outcomes. Identifying myocardium at risk may help direct appropriate patients toward early invasive management.
Figures
Comment in
-
Cardiac magnetic resonance measurements of area at risk and infarct size in ischemic syndromes.J Am Coll Cardiol. 2010 Jun 1;55(22):2489-90. doi: 10.1016/j.jacc.2010.01.048. J Am Coll Cardiol. 2010. PMID: 20510216 No abstract available.
References
-
- Faxon DP. Early reerfusion strategies after acute ST-segment elevation myocardial infarction: the imortance of timing. Nat Clin Pract Cardiovasc Med. 2005;2:22–8. - PubMed
-
- Braunwald E. Alication of current guidelines to the management of unstable angina and non-ST-elevation myocardial infarction. Circulation. 2003;108:III28–37. - PubMed
-
- Rosamond W, Flegal K, Furie K, et al. Heart Disease and Stroke Statistics 2008 Udate. A report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2008;117:e25–146. - PubMed
-
- Hoenig MR, Doust JA, Aroney CN, Scott IA. Early invasive versus conservative strategies for unstable angina & non-ST-elevation myocardial infarction in the stent era. Cochrane Database Syst Rev. 2006;3:CD004815. - PubMed
-
- Anderson JL, Adams CD, Antman EM, et al. ACC/AHA 2007 guidelines for the management of atients with unstable angina/non–ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non-ST-Elevation Myocardial Infarction) J Am Coll Cardiol. 2007;50:e1–157. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
