

Hyperferritinaemia-cataract syndrome: worldwide mutations and phenotype of an increasingly diagnosed genetic disorder
- PMID: 20511138
- PMCID: PMC3525215
- DOI: 10.1186/1479-7364-4-4-250
Hyperferritinaemia-cataract syndrome: worldwide mutations and phenotype of an increasingly diagnosed genetic disorder
Abstract
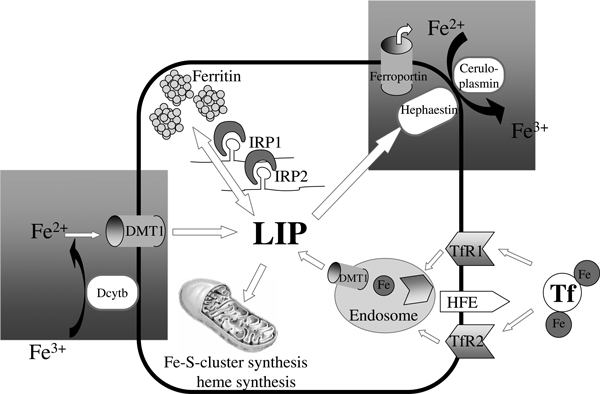
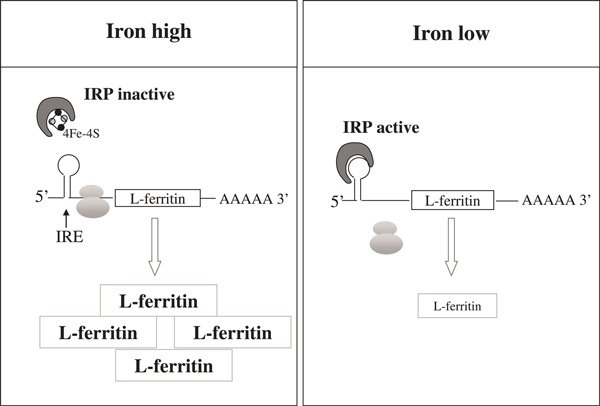
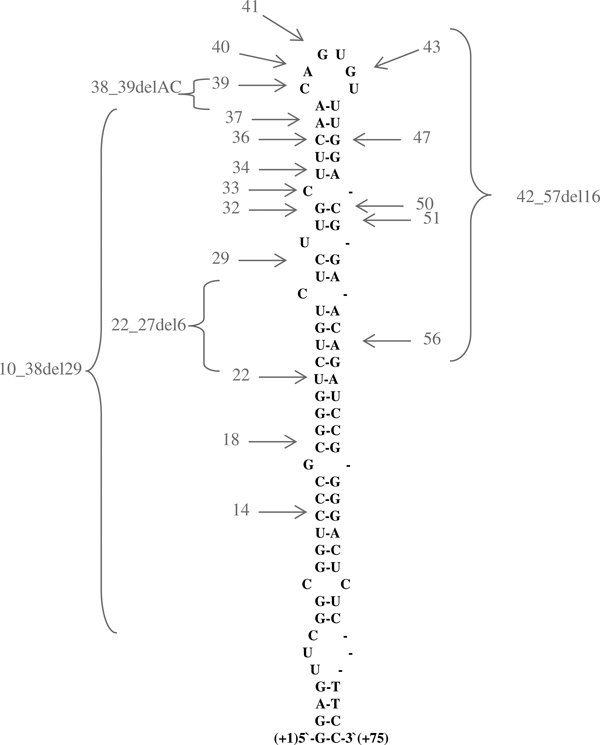
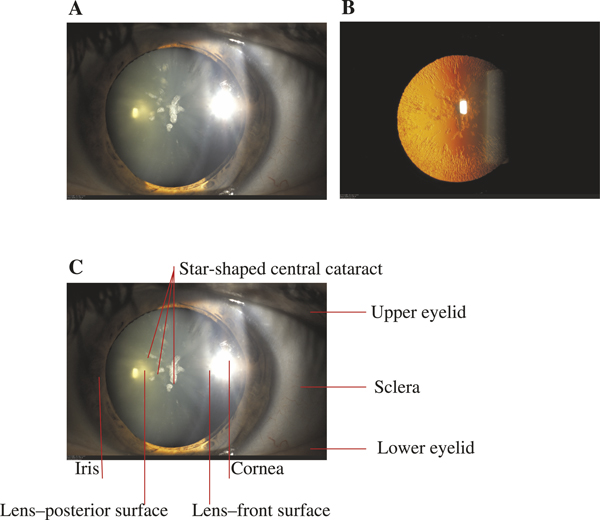
The hereditary hyperferritinaemia-cataract syndrome (HHCS) is characterised by an autosomal dominant cataract and high levels of serum ferritin without iron overload. The cataract develops due to L-ferritin deposits in the lens and its pulverulent aspect is pathognomonic. The syndrome is caused by mutations within the iron-responsive element of L-ferritin. These mutations prevent efficient binding of iron regulatory proteins 1 and 2 to the IRE in L-ferritin mRNA, resulting in an unleashed ferritin translation. This paper reviews all 31 mutations (27 single nucleotide transitions and four deletions) that have been described since 1995. Laboratory test showing hyperferritinaemia, normal serum iron and normal transferrin saturation are indicative for HHCS after exclusion of other causes of increased ferritin levels (inflammation, malignancy, alcoholic liver disease) and should prompt an ophthalmological consultation for diagnostic confirmation. Invasive diagnostics such as liver biopsy are not indicated. HHCS is an important differential diagnosis of hyperferritinaemia. Haematologists, gastroenterologists and ophthalmologists should be aware of this syndrome to spare patients from further invasive diagnosis (liver biopsy), and also from a false diagnosis of hereditary haemochromatosis followed by venesections. Patients diagnosed with HHCS should be counselled regarding the relative harmlessness of this genetic disease, with early cataract surgery as the only clinical consequence.
Figures
References
-
- Frausto da Silva JJR, Williams RJP. The Biological Chemistry of the Elements: The Inorganic Chemistry of Life. Clarendon Press, Oxford, UK; 1991.
-
- Halliwell B, Gutteridge JMC. 'Role of free radicals and catalytic metal ions in human disease: An overview'. Methods Enzymol. 1990;186:1–85. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
