

A clinically relevant orthotopic xenograft model of ependymoma that maintains the genomic signature of the primary tumor and preserves cancer stem cells in vivo
- PMID: 20511191
- PMCID: PMC2940646
- DOI: 10.1093/neuonc/nop056
A clinically relevant orthotopic xenograft model of ependymoma that maintains the genomic signature of the primary tumor and preserves cancer stem cells in vivo
Abstract
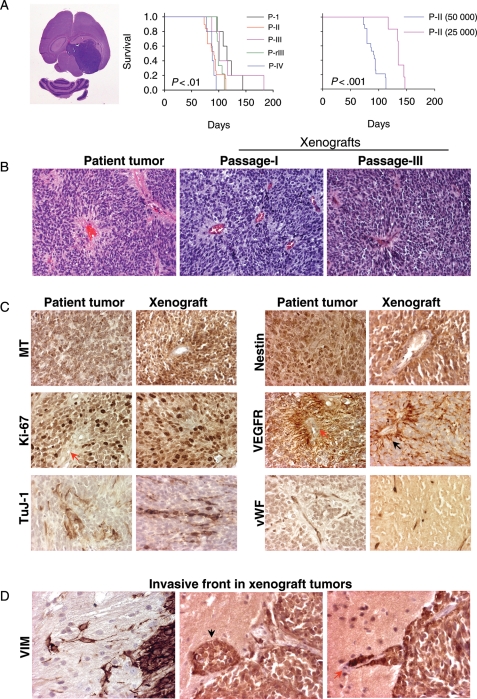
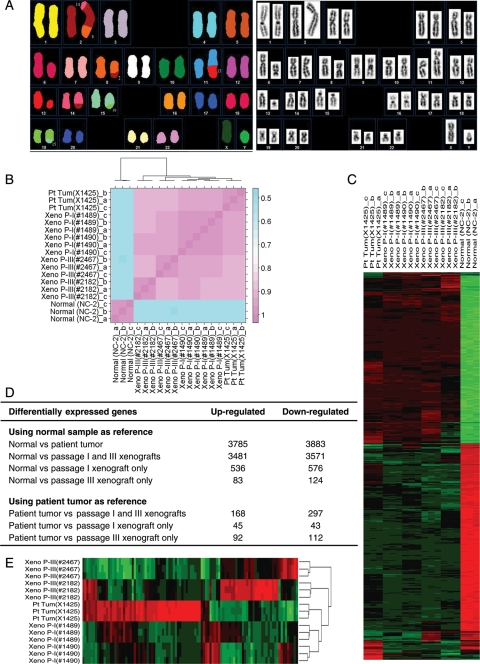
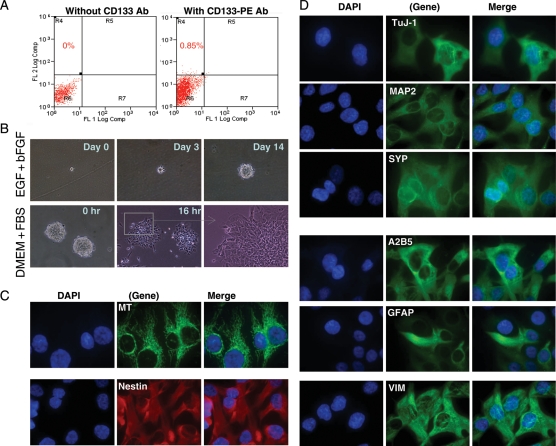
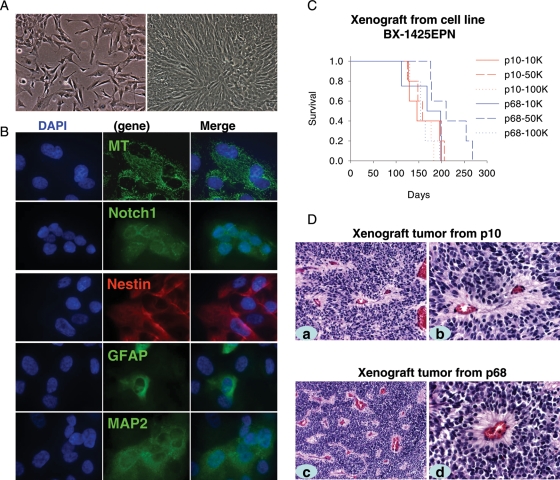
Limited availability of in vitro and in vivo model systems has hampered efforts to understand tumor biology and test novel therapies for ependymoma, the third most common malignant brain tumor that occurs in children. To develop clinically relevant animal models of ependymoma, we directly injected a fresh surgical specimen from a 9-year-old patient into the right cerebrum of RAG2/severe complex immune deficiency (SCID) mice. All five mice receiving the initial transplantation of the patient tumor developed intracerebral xenografts, which have since been serially subtransplanted in vivo in mouse brains for 4 generations and can be cryopreserved for long-term maintenance of tumorigenicity. The xenograft tumors shared nearly identical histopathological features with the original tumors, harbored 8 structural chromosomal abnormalities as detected with spectral karyotyping, maintained gene expression profiles resembling that of the original patient tumor with the preservation of multiple key genetic abnormalities commonly found in human ependymomas, and contained a small population (<2.2%) of CD133(+) stem cells that can form neurospheres and display multipotent capabilities in vitro. The permanent cell line (BXD-1425EPN), which was derived from a passage II xenograft tumor and has been passaged in vitro more than 70 times, expressed similar differentiation markers of the xenograft tumors, maintained identical chromosomal abnormalities, and formed tumors in the brains of SCID mice. In conclusion, direct injection of primary ependymoma tumor cells played an important role in the generation of a clinically relevant mouse model IC-1425EPN and a novel cell line, BXD-1425EPN. This cell line and model will facilitate the biological studies and preclinical drug screenings for pediatric ependymomas.
Figures
Comment in
-
Tumor-initiating cells: an influential paradigm for xenograft research.Neuro Oncol. 2010 Jun;12(6):519. doi: 10.1093/neuonc/noq053. Neuro Oncol. 2010. PMID: 20530515 Free PMC article. No abstract available.
References
-
- Duncan JA, III, Hoffman HJ. Intracranial ependymomas. In: Kaye AH, Lows ERJ, editors. Brain Tumors. Edinburgh: Churchill Livingstone; 1995. pp. 493–504.
-
- Kleihues P, Louis DN, Scheithauer BW, et al. The WHO classification of tumors of the nervous system. J Neuropathol Exp Neurol. 2002;61:215–225. - PubMed
-
- Merchant TE, Mulhern RK, Krasin MJ, et al. Preliminary results from a phase II trial of conformal radiation therapy and evaluation of radiation-related CNS effects for pediatric patients with localized ependymoma. J Clin Oncol. 2004;22:3156–3162. - PubMed
-
- Foreman NK, Love S, Thorne R. Intracranial ependymomas: analysis of prognostic factors in a population-based series. Pediatr Neurosurg. 1996;24:119–125. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
