

Long-term maintenance treatment of restless legs syndrome with gabapentin enacarbil: a randomized controlled study
- PMID: 20511481
- PMCID: PMC2878254
- DOI: 10.4065/mcp.2009.0700
Long-term maintenance treatment of restless legs syndrome with gabapentin enacarbil: a randomized controlled study
Erratum in
- Mayo Clin Proc. 2010 Jul;85(7):693-4
Abstract
Objective: To assess maintenance of efficacy and tolerability of gabapentin enacarbil in patients with moderate to severe primary restless legs syndrome (RLS).
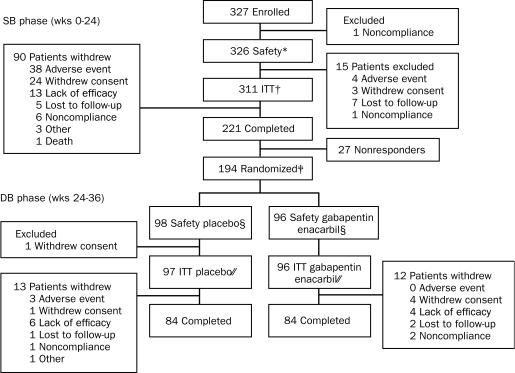
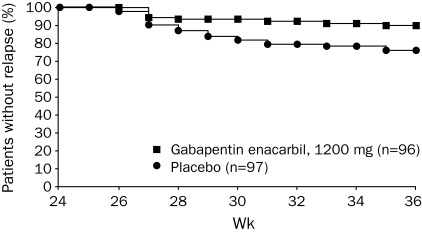
Patients and methods: This study (conducted April 18, 2006, to November 14, 2007) comprised a 24-week, single-blind (SB) treatment phase (gabapentin enacarbil, 1200 mg) followed by a 12-week randomized, double-blind (DB) phase. Responders from the SB phase (patients with improvements on the International Restless Legs Scale [IRLS] and investigator-rated Clinical Global Impression-Improvement scale at week 24 and stable while taking a gabapentin enacarbil dose of 1200 mg for at least 1 month before randomization) were randomized to gabapentin enacarbil, 1200 mg, or placebo once daily at 5 pm with food. The primary end point was the proportion of patients experiencing relapse (worse scores on the IRLS and investigator-rated Clinical Global Impression of Change scale on 2 consecutive visits at least 1 week apart or withdrawal because of lack of efficacy) during the DB phase.
Results: A total of 221 of 327 patients completed the SB phase, 194 (96 in the gabapentin enacarbil group and 98 in the placebo group) were randomized to DB treatment, and 168 (84 in the gabapentin enacarbil group and 84 in the placebo group) completed the DB phase. A significantly smaller proportion of patients treated with gabapentin enacarbil (9/96 [9%]) experienced relapse compared with the placebo-treated patients (22/97 [23%]) (odds ratio, 0.353; 95% confidence interval, 0.2-0.8; P=.02). Somnolence and dizziness were the most common adverse events. One death occurred (unintentional choking during the SB phase) and was judged as being unrelated to the study drug. No clinically relevant changes were observed in laboratory values, in vital signs, or on electrocardiograms.
Conclusion: Gabapentin enacarbil, 1200 mg, maintained improvements in RLS symptoms compared with placebo and showed long-term tolerability in adults with moderate to severe primary RLS for up to 9 months of treatment.
Trial registration: ClinicalTrials.gov NCT00311363.
Figures
Comment in
-
New uses for older drugs: the tales of aspirin, thalidomide, and gabapentin.Mayo Clin Proc. 2010 Jun;85(6):508-11. doi: 10.4065/mcp.2010.0267. Mayo Clin Proc. 2010. PMID: 20511480 Free PMC article. No abstract available.
References
-
- Allen RP, Picchietti D, Hening WA, Trenkwalder C, Walters AS, Montplaisir J. Restless legs syndrome: diagnostic criteria, special considerations, and epidemiology: a report from the restless legs syndrome diagnosis and epidemiology workshop at the National Institutes of Health. Sleep Med. 2003;4(2):101-119 - PubMed
-
- Allen RP, Walters AS, Montplaisir J, et al. Restless legs syndrome prevalence and impact: REST general population study. Arch Intern Med. 2005;165(11):1286-1292 - PubMed
-
- Hening W, Walters AS, Allen RP, Montplaisir J, Myers A, Ferini-Strambi L. Impact, diagnosis and treatment of restless legs syndrome (RLS) in a primary care population: the REST (RLS epidemiology, symptoms, and treatment) primary care study. Sleep Med. 2004;5(3):237-246 - PubMed
-
- Kushida CA, Allen RP, Atkinson MJ. Modeling the causal relationships between symptoms associated with restless legs syndrome and the patient-reported impact of RLS. Sleep Med. 2004;5(5):485-488 - PubMed
-
- Winkelman JW, Johnston L. Augmentation and tolerance with long-term pramipexole treatment of restless legs syndrome (RLS). Sleep Med. 2004;5(1):9-14 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
