

Severe kyphoscoliosis after primary Echinococcus granulosus infection of the spine
- PMID: 20514501
- PMCID: PMC2989289
- DOI: 10.1007/s00586-010-1398-6
Severe kyphoscoliosis after primary Echinococcus granulosus infection of the spine
Abstract
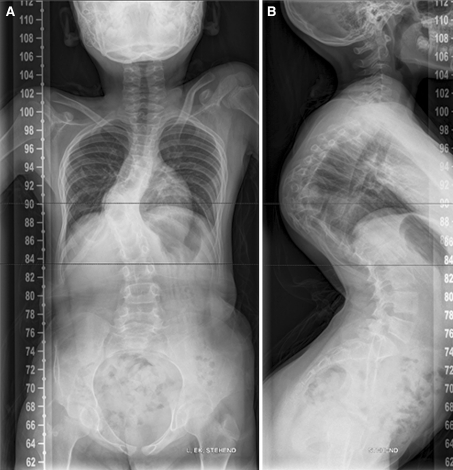
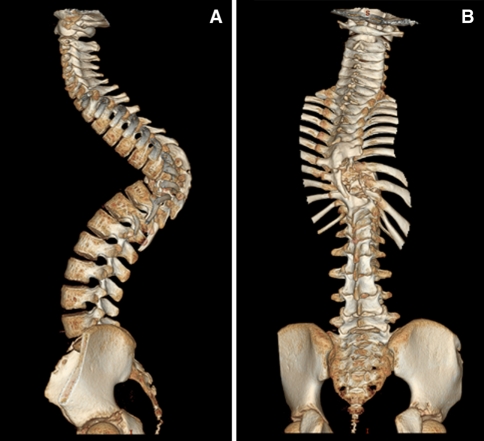
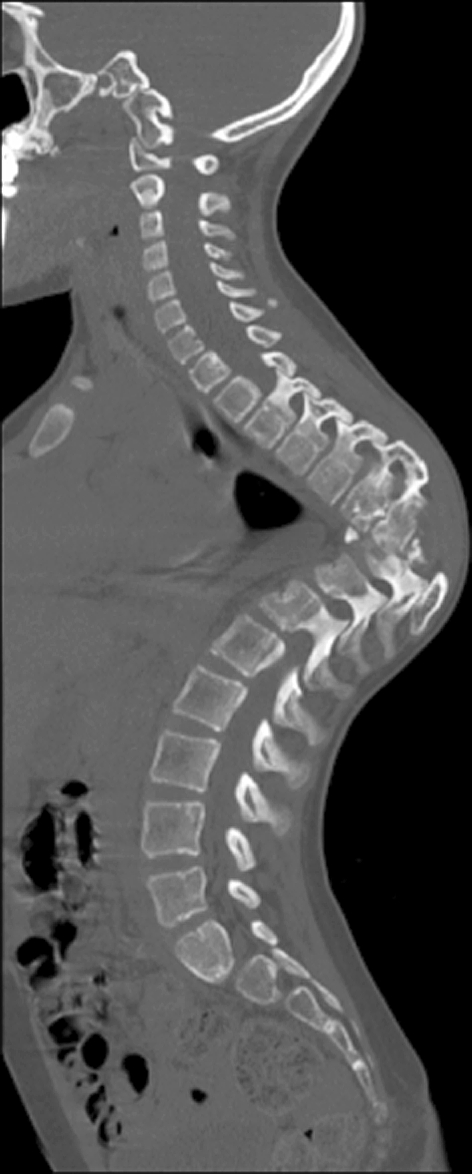
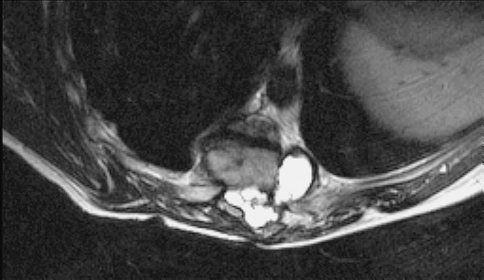
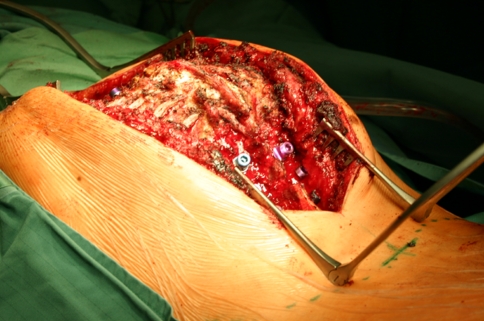
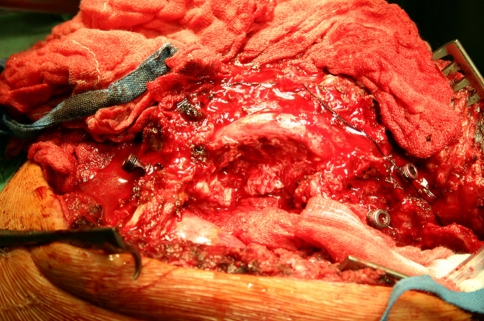
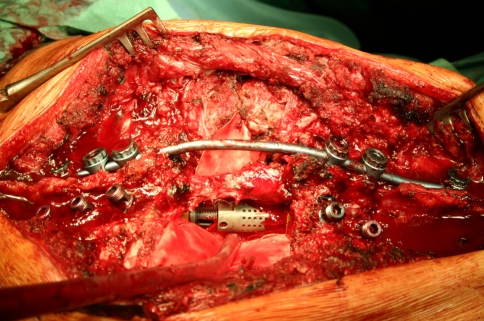
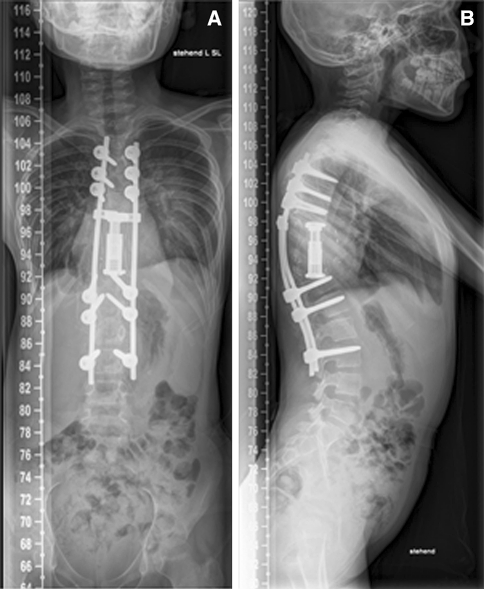
A primary Echinococcus granulosus infection of the spine involving the vertebrae T8 and T9 of a 6-year-old child was treated elsewhere by thoracotomy, partial corporectomy, multiple laminectomies and uninstrumented fusion. Owing to inappropriate stabilization, severe deformity developed secondary to these surgeries. X-rays, CT and MRI scans of the spine revealed a severe thoracic kyphoscoliosis of more than 100 degrees (Fig. 1) and recurrence of Echinococcus granulosus infection. The intraspinal cyst formation was located between the stretched dural sac and the vertebral bodies of the kyphotic apex causing significant compression of the cord (Figs. 2, 3, 4). A progressive neurologic deficit was reported by the patient. At the time of referral, the patient was wheelchair bound and unable to walk by herself (Frankel Grade C). Standard antiinfectious therapy of Echinococcus granulosus requires a minimum treatment period of 3 months. This should be done before any surgical intervention because in case of a rupture of an active cyst, the delivered lipoprotein antigens of the parasite may cause a potentially lethal anaphylactic shock. Owing to the critical neurological status, we decided to perform surgery without full length preoperative antiinfectious therapy. Surgical treatment consisted in posterior vertebral column resection technique with an extensive bilateral costotransversectomy over three levels, re-decompression with cyst excision around the apex and multilevel corporectomy of the apex of the deformity. Stabilisation and correction of the spinal deformity were done by insertion of a vertebral body replacement cage anteriorly and posterior shortening by compression and by a multisegmental pedicle screw construct. After the surgery, antihelminthic therapy was continued. The patients neurological deficits resolved quickly: 4 weeks after surgery, the patient had Frankel Grade D and was ambulatory without any assistance. After an 18-month follow-up, the patient is free of recurrence of infection and free of neurologically deficits (Frankel E). This case demonstrates that inappropriate treatment--partial resection of the cyst, inappropriate anterior stabilization and posterior multilevel laminectomies without posterior stabilization--may lead to severe progressive kyphoscoliotic deformity and recurrence of infection, both leading to significant neurological injury presenting as a very difficult to treat pathology. Fig. 1 X-rays of the patient showing a kyhoscoliotic deformity. a ap view, b lateral view Fig. 2 CT reconstruction of the whole spine showing the apex of the deformity is located in the area of the previous surgeries Fig. 3 Sagittal CT-cut showing the bone bloc at the apex with a translation deformity Fig. 4 Sagittal T2-weighted MRI image showing the cystic formation at the apex.
Figures




Comment in
-
Expert's comment concerning Grand Rounds case entitled "Severe Kyphoscoliosis after primary echinococcus granulosus infection of the spine" (by M. Thaler, M. Gabl, R. Lechner, M. Gstöttner and C.M. Bach).Eur Spine J. 2010 Sep;19(9):1423-4. doi: 10.1007/s00586-010-1408-8. Epub 2010 Jun 8. Eur Spine J. 2010. PMID: 20532574 Free PMC article. No abstract available.
References
-
- Bhojraj SY, Shetty NR. Primary hydatid disease of the spine: an unusual cause of progressive paraplegia: case report and review of the literature. J Neurosurg. 1999;91:216–218. - PubMed
-
- Braithwaite PA, Lees RF. Vertebral hydatid disease: radiological assessment. Radiology. 1981;140:763–766. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
