

Cognitive behavioral guided self-help for the treatment of recurrent binge eating
- PMID: 20515207
- PMCID: PMC2880824
- DOI: 10.1037/a0018915
Cognitive behavioral guided self-help for the treatment of recurrent binge eating
Abstract
Objective: Despite proven efficacy of cognitive behavioral therapy (CBT) for treating eating disorders with binge eating as the core symptom, few patients receive CBT in clinical practice. Our blended efficacy-effectiveness study sought to evaluate whether a manual-based guided self-help form of CBT (CBT-GSH), delivered in 8 sessions in a health maintenance organization setting over a 12-week period by master's-level interventionists, is more effective than treatment as usual (TAU).
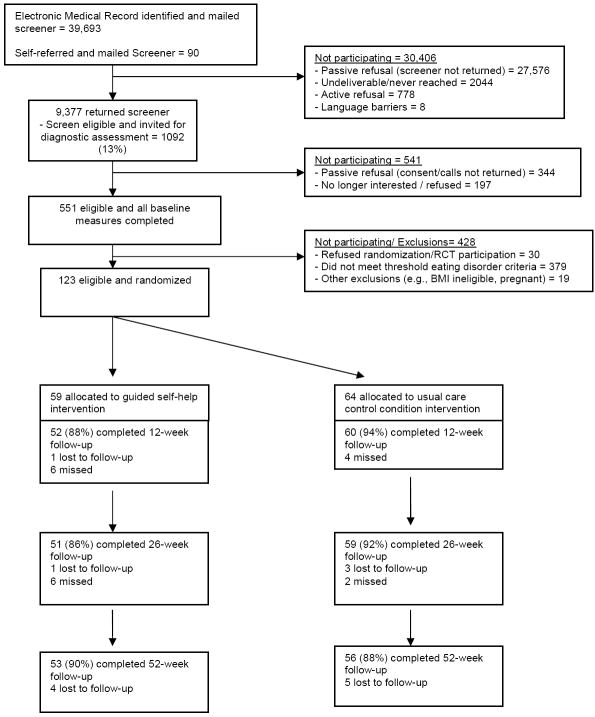
Method: In all, 123 individuals (mean age = 37.2; 91.9% female, 96.7% non-Hispanic White) were randomized, including 10.6% with bulimia nervosa (BN), 48% with binge eating disorder (BED), and 41.4% with recurrent binge eating in the absence of BN or BED. Baseline, posttreatment, and 6- and 12-month follow-up data were used in intent-to-treat analyses.
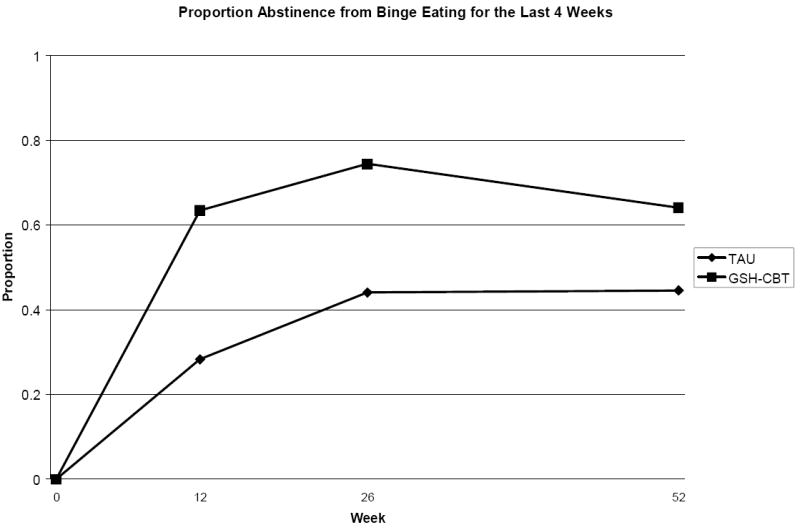
Results: At 12-month follow-up, CBT-GSH resulted in greater abstinence from binge eating (64.2%) than TAU (44.6%; number needed to treat = 5), as measured by the Eating Disorder Examination (EDE). Secondary outcomes reflected greater improvements in the CBT-GSH group in dietary restraint (d = 0.30); eating, shape, and weight concern (ds = 0.54, 1.01, 0.49, respectively; measured by the EDE Questionnaire); depression (d = 0.56; Beck Depression Inventory); and social adjustment (d = 0.58; Work and Social Adjustment Scale), but not weight change.
Conclusions: CBT-GSH is a viable first-line treatment option for the majority of patients with recurrent binge eating who do not meet diagnostic criteria for BN or anorexia nervosa.
Figures
Similar articles
-
Cost-effectiveness of guided self-help treatment for recurrent binge eating.J Consult Clin Psychol. 2010 Jun;78(3):322-33. doi: 10.1037/a0018982. J Consult Clin Psychol. 2010. PMID: 20515208 Free PMC article. Clinical Trial.
-
Web-Based Cognitive Behavioral Therapy for Female Patients With Eating Disorders: Randomized Controlled Trial.J Med Internet Res. 2015 Jun 18;17(6):e152. doi: 10.2196/jmir.3946. J Med Internet Res. 2015. PMID: 26088580 Free PMC article. Clinical Trial.
-
Treatment of binge eating disorder.Psychiatr Clin North Am. 2011 Dec;34(4):773-83. doi: 10.1016/j.psc.2011.08.011. Epub 2011 Oct 5. Psychiatr Clin North Am. 2011. PMID: 22098803
-
The Efficacy of Psychological Therapies in Reducing Weight and Binge Eating in People with Bulimia Nervosa and Binge Eating Disorder Who Are Overweight or Obese-A Critical Synthesis and Meta-Analyses.Nutrients. 2017 Mar 17;9(3):299. doi: 10.3390/nu9030299. Nutrients. 2017. PMID: 28304341 Free PMC article. Review.
-
Meta-analysis of the effects of cognitive-behavioral therapy on the core eating disorder maintaining mechanisms: implications for mechanisms of therapeutic change.Cogn Behav Ther. 2018 Mar;47(2):107-125. doi: 10.1080/16506073.2018.1427785. Epub 2018 Jan 30. Cogn Behav Ther. 2018. PMID: 29378481 Review.
Cited by
-
Psychological treatments for binge eating disorder.Curr Psychiatry Rep. 2012 Aug;14(4):432-46. doi: 10.1007/s11920-012-0277-8. Curr Psychiatry Rep. 2012. PMID: 22707016 Free PMC article. Review.
-
Randomized controlled trial comparing smartphone assisted versus traditional guided self-help for adults with binge eating.Int J Eat Disord. 2017 Nov;50(11):1313-1322. doi: 10.1002/eat.22781. Epub 2017 Sep 27. Int J Eat Disord. 2017. PMID: 28960384 Free PMC article. Clinical Trial.
-
The role of impulsivity and binge eating in outpatients with overweight or obesity: an EEG temporal discounting study.J Eat Disord. 2024 Sep 3;12(1):130. doi: 10.1186/s40337-024-01080-2. J Eat Disord. 2024. PMID: 39227881 Free PMC article.
-
Perceptions of the feasibility and acceptability of a smartphone application for the treatment of binge eating disorders: Qualitative feedback from a user population and clinicians.Int J Med Inform. 2015 Oct;84(10):808-16. doi: 10.1016/j.ijmedinf.2015.06.004. Epub 2015 Jun 15. Int J Med Inform. 2015. PMID: 26113461 Free PMC article.
-
Binge-eating disorder diagnosis and treatment: a recap in front of DSM-5.BMC Psychiatry. 2015 Apr 3;15:70. doi: 10.1186/s12888-015-0445-6. BMC Psychiatry. 2015. PMID: 25885566 Free PMC article. Review.
References
-
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4. Washington DC: Author; 2000.
-
- Banasiak SJ, Paxton SJ, Hay PJ. Perceptions of cognitive behavioural guided self-help treatment for bulimia nervosa in primary care. Eating Disorders. 2007;15(1):23–40. - PubMed
-
- Beck AT, Steer RA, Garbin MG. Psychometric properties of the Beck depression Inventory: Twenty-five years of evaluation. Clinical Psychology Review. 1988;8(1):77–100.
-
- Brownley KA, Berkman ND, Sedway JA, Lohr KN, Bulik CM. Binge eating disorder treatment: A systematic review of randomized controlled trials. International Journal of Eating Disorders. 2007;40(4):337–348. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
