

Second-opinion stress tele-echocardiography for the Adonhers (Aged donor heart rescue by stress echo) project
- PMID: 20515476
- PMCID: PMC2887413
- DOI: 10.1186/1476-7120-8-20
Second-opinion stress tele-echocardiography for the Adonhers (Aged donor heart rescue by stress echo) project
Abstract
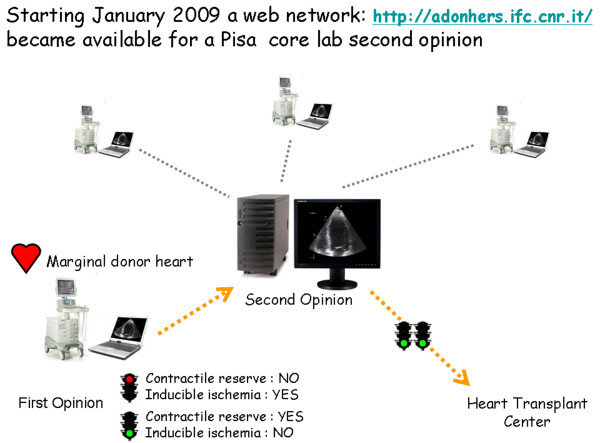
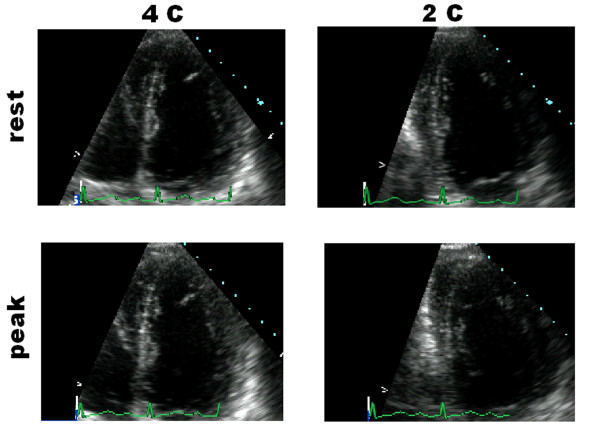
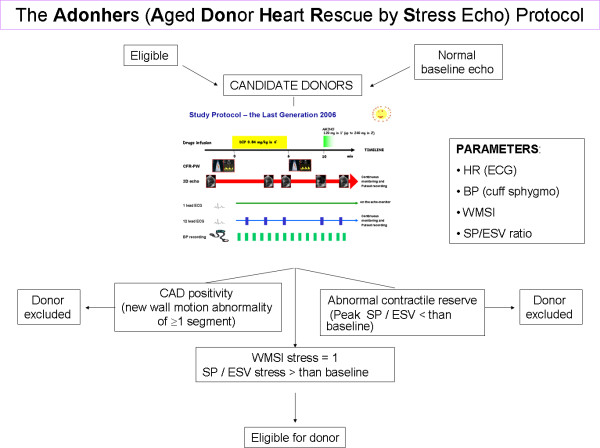
Background: To resolve the current shortage of donor hearts, we established the Adonhers protocol. An upward shift of the donor age cut-off limit (from the present 55 to 65 years) is acceptable if a stress echo screening on the candidate donor heart is normal. This study aimed to verify feasibility of a "second opinion" of digitally transferred images of stress echo results to minimize technical variability in selection of aged donor hearts for heart transplant.
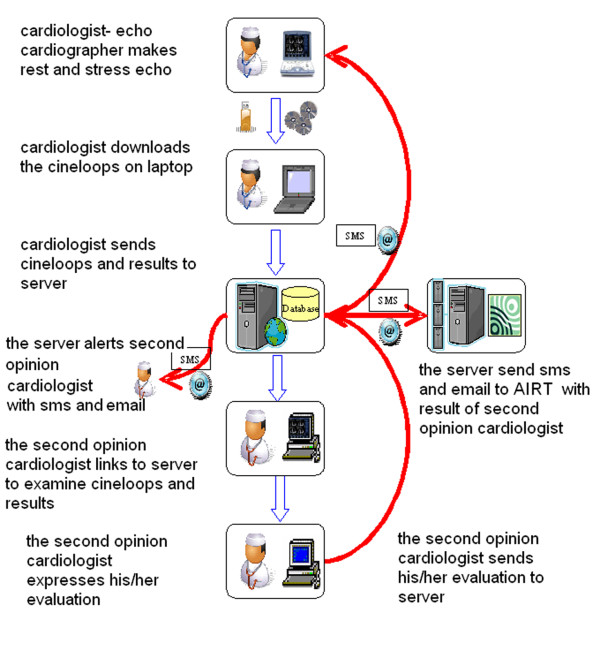
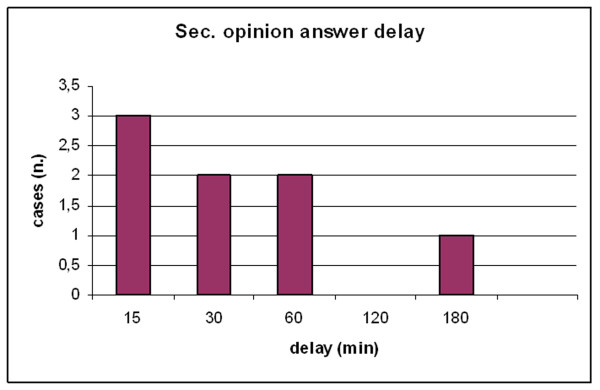
Methods: The informatics infrastructure was created for a core lab reading with a second opinion from the Pisa stress echo lab. To test the system, simulation standard stress echo cineloops were sent digitally from 5 peripheral labs to the central core lab.Starting January 2009, real marginal donor stress echos were sent via internet to the central core echo lab, Pisa, for a second opinion before heart transplant.
Results: In the simulation protocol, 30 dipyridamole stress echocardiograms were sent from the five peripheral echo labs to the central core lab in Pisa. Both the echo images and reports were correctly uploaded in the web system and sent to the core echo lab; the second opinion evaluation was obtained in all cases (100% feasibility). In the transplant protocol, eight donor cases were sent to the Pisa core lab for the second opinion protocol, and six of them were transplanted in marginal recipients.
Conclusions: Second-Opinion Stress Tele-Echocardiography can effectively be performed in a network aimed to safely expand the heart donor pool for heart transplant.
Figures
References
-
- Leone O, Gherardi S, Targa L, Pasanisi E, Mikus P, Tanganelli P, Maccherini M, Arpesella G, Picano E, Bombardini T. Stress echocardiography as a gatekeeper to donation in aged marginal donor hearts: anatomic and pathologic correlations of abnormal stress echocardiography results. J Heart Lung Transplant. 2009;28:1141–9. doi: 10.1016/j.healun.2009.05.029. - DOI - PubMed
-
- Zaroff JG, Rosengard BR, Armstrong WF, Babcock WD, D'Alessandro A, Dec GW, Edwards NM, Higgins RS, Jeevanandum V, Kauffman M, Kirklin JK, Large SR, Marelli D, Peterson TS, Ring WS, Robbins RC, Russell SD, Taylor DO, Van Bakel A, Wallwork J, Young JB. Consensus conference report: maximizing use of organs received from cadaver donor-cardiac recommendations, , March 28-29, 2001, Crystal City, VA. Circulation. 2002;106:836–41. doi: 10.1161/01.CIR.0000025587.40373.75. - DOI - PubMed
-
- The U.S. Organ Procurement and Transplantation Network and the Scientific Registry of Transplant Recipients. OPTN/SRTR- data. 2008. - PubMed
-
- Picano E. Stress echocardiography: from pathophysiological toy to diagnostic tool. Point of view. Circulation. 1992;85:1604–12. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
