

Effects of four different meal types on the population pharmacokinetics of single-dose rifapentine in healthy male volunteers
- PMID: 20516273
- PMCID: PMC2916304
- DOI: 10.1128/AAC.00345-10
Effects of four different meal types on the population pharmacokinetics of single-dose rifapentine in healthy male volunteers
Abstract
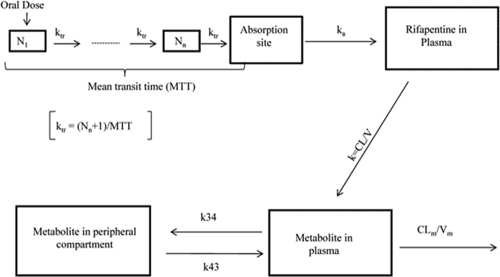
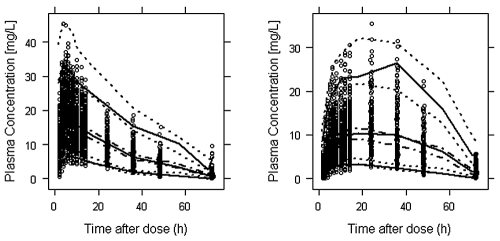
Rifapentine and its primary metabolite, 25-desacetyl rifapentine, are active against mycobacterium tuberculosis. The objectives of this study were to describe the population pharmacokinetics of rifapentine and 25-desacetyl rifapentine in fasting and fed states. Thirty-five male healthy volunteers were enrolled in an open-label, randomized, sequential, five-way crossover study. Participants received a single 900-mg dose of rifapentine after meals with high fat (meal A), bulk and low fat (meal B), bulk and high fat (meal C), high fluid and low fat (meal D), or 200 ml of water (meal E). Venous blood samples were collected over 72 h after each rifapentine dose, and plasma was analyzed for rifapentine and 25-desacetyl rifapentine using high-performance liquid chromatography. Pharmacokinetic data were analyzed by nonlinear mixed-effect modeling using NONMEM. Compared with the fasting state, meal A had the greatest effect on rifapentine oral bioavailability, increasing it by 86%. Meals B, C, and D resulted in 33%, 46%, and 49% increases in rifapentine oral bioavailability, respectively. Similar trends were observed for 25-desacetyl rifapentine. As meal behavior has a substantial impact on rifapentine exposure, it should be considered in the evaluation of optimal dosing approaches.
Figures
Similar articles
-
Rifapentine Population Pharmacokinetics and Dosing Recommendations for Latent Tuberculosis Infection.Am J Respir Crit Care Med. 2020 Sep 15;202(6):866-877. doi: 10.1164/rccm.201912-2489OC. Am J Respir Crit Care Med. 2020. PMID: 32412342 Free PMC article.
-
Pharmacokinetics of rifapentine in subjects seropositive for the human immunodeficiency virus: a phase I study.Antimicrob Agents Chemother. 1999 May;43(5):1230-3. doi: 10.1128/AAC.43.5.1230. Antimicrob Agents Chemother. 1999. PMID: 10223941 Free PMC article. Clinical Trial.
-
Population pharmacokinetics of rifapentine and desacetyl rifapentine in healthy volunteers: nonlinearities in clearance and bioavailability.Antimicrob Agents Chemother. 2014 Jun;58(6):3035-42. doi: 10.1128/AAC.01918-13. Epub 2014 Mar 10. Antimicrob Agents Chemother. 2014. PMID: 24614383 Free PMC article. Clinical Trial.
-
Pharmacokinetics of rifapentine in children.Pediatr Infect Dis J. 2006 May;25(5):405-9. doi: 10.1097/01.inf.0000214963.55217.9c. Pediatr Infect Dis J. 2006. PMID: 16645503
-
Rifampin vs. rifapentine: what is the preferred rifamycin for tuberculosis?Expert Rev Clin Pharmacol. 2017 Oct;10(10):1027-1036. doi: 10.1080/17512433.2017.1366311. Epub 2017 Aug 18. Expert Rev Clin Pharmacol. 2017. PMID: 28803492 Review.
Cited by
-
Rifapentine Population Pharmacokinetics and Dosing Recommendations for Latent Tuberculosis Infection.Am J Respir Crit Care Med. 2020 Sep 15;202(6):866-877. doi: 10.1164/rccm.201912-2489OC. Am J Respir Crit Care Med. 2020. PMID: 32412342 Free PMC article.
-
Official American Thoracic Society/Centers for Disease Control and Prevention/Infectious Diseases Society of America Clinical Practice Guidelines: Treatment of Drug-Susceptible Tuberculosis.Clin Infect Dis. 2016 Oct 1;63(7):e147-e195. doi: 10.1093/cid/ciw376. Epub 2016 Aug 10. Clin Infect Dis. 2016. PMID: 27516382 Free PMC article.
-
Superior Efficacy of a Bedaquiline, Delamanid, and Linezolid Combination Regimen in a Mouse Tuberculosis Model.J Infect Dis. 2021 Sep 17;224(6):1039-1047. doi: 10.1093/infdis/jiab043. J Infect Dis. 2021. PMID: 33502537 Free PMC article.
-
A Phase 2 Randomized Trial of a Rifapentine plus Moxifloxacin-Based Regimen for Treatment of Pulmonary Tuberculosis.PLoS One. 2016 May 9;11(5):e0154778. doi: 10.1371/journal.pone.0154778. eCollection 2016. PLoS One. 2016. PMID: 27159505 Free PMC article. Clinical Trial.
-
Effect of adherence as measured by MEMS, ritonavir boosting, and CYP3A5 genotype on atazanavir pharmacokinetics in treatment-naive HIV-infected patients.Clin Pharmacol Ther. 2012 Nov;92(5):575-83. doi: 10.1038/clpt.2012.137. Epub 2012 Oct 3. Clin Pharmacol Ther. 2012. PMID: 23033116 Free PMC article. Clinical Trial.
References
-
- Beal, S. L., L. B. Sheiner, and A. Boeckmann. 1996. NONMEM users' guides. University of California, San Fransisco, San Francisco, CA.
-
- Blumberg, H. M., W. J. Burman, R. E. Chaisson, C. L. Daley, S. C. Etkind, L. N. Friedman, P. Fujiwara, M. Grzemska, P. C. Hopewell, M. D. Iseman, R. M. Jasmer, V. Koppaka, R. I. Menzies, R. J. O'Brien, R. R. Reves, L. B. Reichman, P. M. Simone, J. R. Starke, and A. A. Vernon. 2003. American Thoracic Society/Centers for Disease Control and Prevention/Infectious Diseases Society of America: treatment of tuberculosis. Am. J. Respir. Crit. Care Med. 167:603-662. - PubMed
-
- Bock, N. N., T. R. Sterling, C. D. Hamilton, C. Pachucki, Y. C. Wang, D. S. Conwell, A. Mosher, M. Samuels, and A. Vernon. 2002. A prospective, randomized, double-blind study of the tolerability of rifapentine 600, 900, and 1,200 mg plus isoniazid in the continuation phase of tuberculosis treatment. Am. J. Respir. Crit. Care Med. 165:1526-1530. - PubMed
-
- Burman, W., D. Benator, A. Vernon, A. Khan, B. Jones, C. Silva, C. Lahart, S. Weis, B. King, B. Mangura, M. Weiner, and W. El-Sadr. 2006. Acquired rifamycin resistance with twice-weekly treatment of HIV-related tuberculosis. Am. J. Respir. Crit. Care Med. 173:350-356. - PubMed
-
- Burman, W. J., K. Gallicano, and C. Peloquin. 2001. Comparative pharmacokinetics and pharmacodynamics of the rifamycin antibacterials. Clin. Pharmacokinet. 40:327-341. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
