

Effect of pregnancy on postural tachycardia syndrome
- PMID: 20516426
- PMCID: PMC2894719
- DOI: 10.4065/mcp.2009.0672
Effect of pregnancy on postural tachycardia syndrome
Abstract
Objectives: To compare the clinical presentation, autonomic dysfunction, and pregnancy outcomes in parous and nulliparous women with postural tachycardia syndrome (POTS) and in women with POTS before and after pregnancy.
Patients and methods: This study consists of women who had at least 1 pregnancy during which time they met criteria for POTS between May 1993 and July 2009. All patients underwent standard autonomic testing. POTS was defined as a heart rate (HR) increase of greater than 30 beats/min on head-up tilt (HUT) with symptoms of orthostatic intolerance. Patients' charts were reviewed retrospectively to determine pregnancy outcomes.
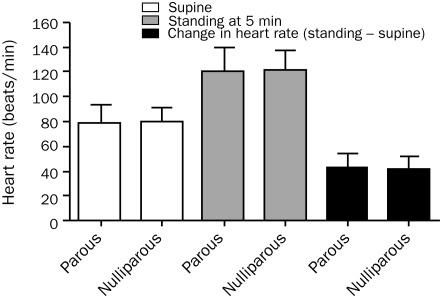
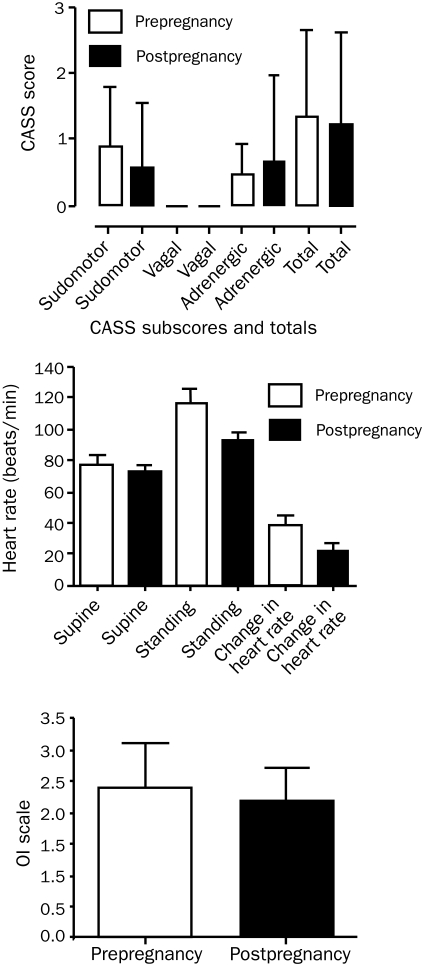
Results: Clinical characteristics related to POTS did not differ between parous and nulliparous women except for disease duration (parous, 3.7+/-2.6; nulliparous, 2.1+/-2.2; P<.001). Autonomic dysfunction did not differ between groups (change in HR on HUT: parous, 42.6+/-12.0 beats/min; nulliparous, 41.3+/-10.6 beats/min; P=.39). Of 116 total pregnancies, adverse pregnancy outcomes were reported in 9% and maternal complications in 1%. No complication was related to POTS. There was a trend toward modest improvement in autonomic dysfunction before and after pregnancy (change in HR on HUT: before pregnancy, 38.1+/-22.7 beats/min; after pregnancy, 21.9+/-14.9 beats/min; P=.07).
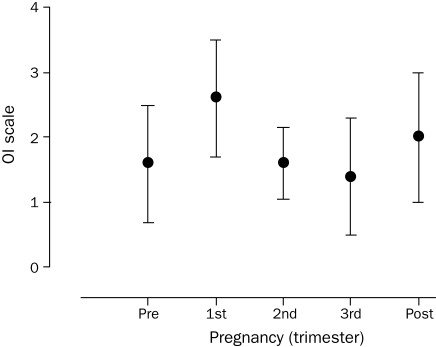
Conclusion: The long-term impact of pregnancy on POTS does not appear to be clinically important. However, there does appear to be a trend toward improvement in the short-term postpartum period. Adverse pregnancy events were similar to those seen in the general public and do not present a barrier to women with POTS who want to have children.
Figures
References
-
- Low PA, Opfer-Gehrking TL, Textor SC, et al. Comparison of the postural tachycardia syndrome (POTS) with orthostatic hypotension due to autonomic failure. J Auton Nerv Syst. 1994;50(2):181-188 - PubMed
-
- Thieben MJ, Sandroni P, Sletten DM, et al. Postural orthostatic tachycardia syndrome: the Mayo Clinic experience. Mayo Clin Proc. 2007;82(3):308-313 - PubMed
-
- Sandroni P, Opfer-Gehrking TL, McPhee BR, Low PA. Postural tachycardia syndrome: clinical features and follow-up study. Mayo Clin Proc. 1999;74(11):1106-1110 - PubMed
-
- Schondorf R, Low PA. Idiopathic postural orthostatic tachycardia syndrome: an attenuated form of acute pandysautonomia? Neurology 1993;43(1):132-137 - PubMed
-
- Jacob G, Costa F, Shannon JR, et al. The neuropathic postural tachycardia syndrome. N Engl J Med. 2000;343(14):1008-1014 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
