

Clinical relevance of microsatellite instability in colorectal cancer
- PMID: 20516444
- PMCID: PMC2903331
- DOI: 10.1200/JCO.2009.27.0652
Clinical relevance of microsatellite instability in colorectal cancer
Abstract
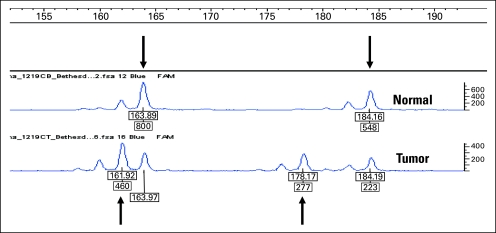
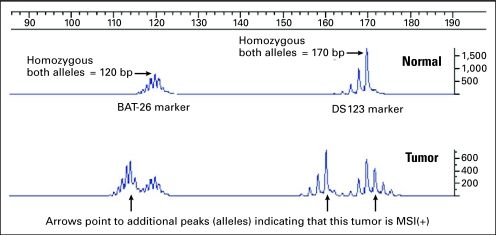
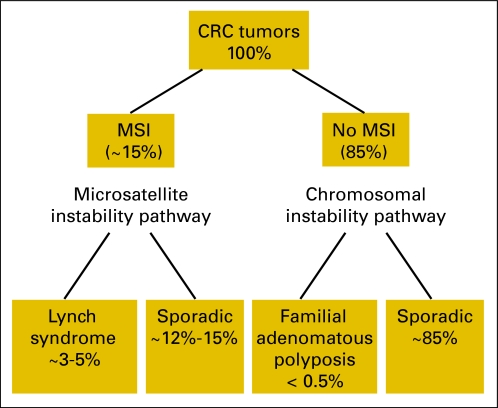
Microsatellite instability (MSI) is a clonal change in the number of repeated DNA nucleotide units in microsatellites. It arises in tumors with deficient mismatch repair due to the inactivation of one of the four mismatch repair genes: MSH2, MLH1, MSH6, and PMS2. In order to determine the MSI status of a tumor, microdissection and polymerase chain reaction-based detection strategies are required. For practical purposes, MSI is equivalent to the loss of staining by immunohistochemistry (IHC) of one of the mismatch repair genes since both signify an abnormality in mismatch repair. Of all colorectal cancers (CRCs), 15% to 20% display MSI or abnormal IHC (often referred to as microsatellite instability [MIN] pathway). The remaining 80% to 85% of CRCs are microsatellite stable but most are characterized by chromosomal instability (CIN pathway). Almost all Lynch syndrome tumors have MSI or abnormal IHC and they account for up to one third of all MIN CRCs (3% to 5% of all CRCs). The remaining MIN tumors are sporadic as a result of somatic inactivation of the MLH1 gene caused by methylation of its promoter. Thus, the presence of a MSI/IHC abnormality prompts further investigations to diagnose Lynch syndrome, whereas its absence excludes Lynch syndrome. We recommend screening all CRC tumors for IHC or MSI. MIN tumors have a more favorable outcome than CIN tumors, and fluorouracil-based adjuvant chemotherapy does not improve the outcome of stage II or stage III MIN tumors. More data are needed to determine how best to treat patients with stage II and stage III MIN CRCs.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
References
-
- Pasche B, Luo Y, Rao PH, et al. Type I transforming growth factor ß receptor maps to 9q22 and exhibits a polymorphism and a rare variant within a polyalanine tract. Cancer Res. 1998;58:2727–2732. - PubMed
-
- Markowitz S, Wang J, Myeroff L, et al. Inactivation of the type II TGF-ß receptor in colon cancer cells with microsatellite instability. Science. 1995;268:1336–1338. - PubMed
-
- Rampino N, Yamamoto H, Ionov Y, et al. Somatic frameshift mutations in the BAX gene in colon cancers of the microsatellite mutator phenotype. Science. 1997;275:967–969. - PubMed
-
- Hienonen T, Sammalkorpi H, Enholm S, et al. Mutations in two short noncoding mononucleotide repeats in most microsatellite-unstable colorectal cancers. Cancer Res. 2005;65:4607–4612. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
