

Longitudinal study of vision and retinal nerve fiber layer thickness in multiple sclerosis
- PMID: 20517936
- PMCID: PMC2901775
- DOI: 10.1002/ana.22005
Longitudinal study of vision and retinal nerve fiber layer thickness in multiple sclerosis
Abstract
Objective: Cross-sectional studies of optical coherence tomography (OCT) show that retinal nerve fiber layer (RNFL) thickness is reduced in multiple sclerosis (MS) and correlates with visual function. We determined how longitudinal changes in RNFL thickness relate to visual loss. We also examined patterns of RNFL thinning over time in MS eyes with and without a prior history of acute optic neuritis (ON).
Methods: Patients underwent OCT measurement of RNFL thickness at baseline and at 6-month intervals during a mean follow-up of 18 months at 3 centers. Low-contrast letter acuity (2.5%, 1.25% contrast) and visual acuity (VA) were assessed.
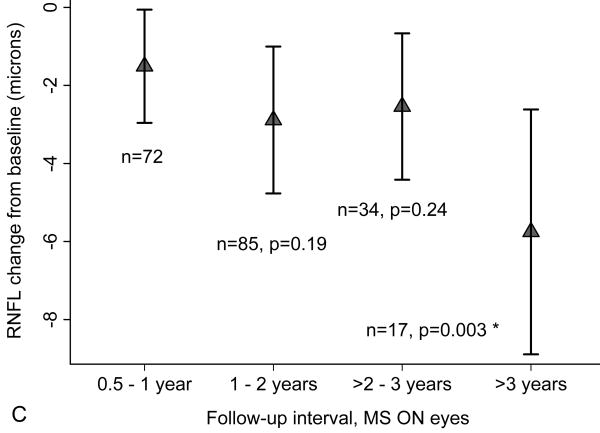
Results: Among 299 patients (593 eyes) with >or=6 months follow-up, eyes with visual loss showed greater RNFL thinning compared to eyes with stable vision (low-contrast acuity, 2.5%: p < 0.001; VA: p = 0.005). RNFL thinning increased over time, with average losses of 2.9microm at 2 to 3 years and 6.1microm at 3 to 4.5 years (p < 0.001 vs 0.5-1-year follow-up interval). These patterns were observed for eyes with or without prior history of ON. Proportions of eyes with RNFL loss greater than test-retest variability (>or=6.6microm) increased from 11% at 0 to 1 year to 44% at 3 to 4.5 years (p < 0.001).
Interpretation: Progressive RNFL thinning occurs as a function of time in some patients with MS, even in the absence of ON, and is associated with clinically significant visual loss. These findings are consistent with subclinical axonal loss in the anterior visual pathway in MS, and support the use of OCT and low-contrast acuity as methods to evaluate the effectiveness of putative neuroprotection protocols.
Figures






References
-
- Mowry EM, Loguidice MJ, Daniels AB, et al. Vision related quality of life in multiple sclerosis: correlation with new measures of low and high contrast letter acuity. J Neurol Neurosurg Psychiatry. 2009;80:767–772. - PubMed
-
- Trapp BD, Peterson J, Ransohoff RM, et al. Axonal transection in the lesions of multiple sclerosis. N Engl J Med. 1998;338:278–285. - PubMed
-
- Evangelou N, Konz D, Esiri MM, et al. Size-selective neuronal changes in the anterior optic pathways suggest a differential susceptibility to injury in multiple sclerosis. Brain. 2001;124:1813–1820. - PubMed
-
- DeLuca GC, Williams K, Evangelou N, et al. The contribution of demyelination to axonal loss in multiple sclerosis. Brain. 2006;129:1507–1516. - PubMed
-
- Sepulcre J, Goñi J, Masdeu JC, et al. Contribution of white matter lesions to gray matter atrophy in multiple sclerosis: evidence from voxel-based analysis of T1 lesions in the visual pathway. Arch Neurol. 2009;66:173–179. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
