

Noninvasive autoregulation monitoring with and without intracranial pressure in the naive piglet brain
- PMID: 20519421
- PMCID: PMC5505736
- DOI: 10.1213/ANE.0b013e3181e054ba
Noninvasive autoregulation monitoring with and without intracranial pressure in the naive piglet brain
Abstract
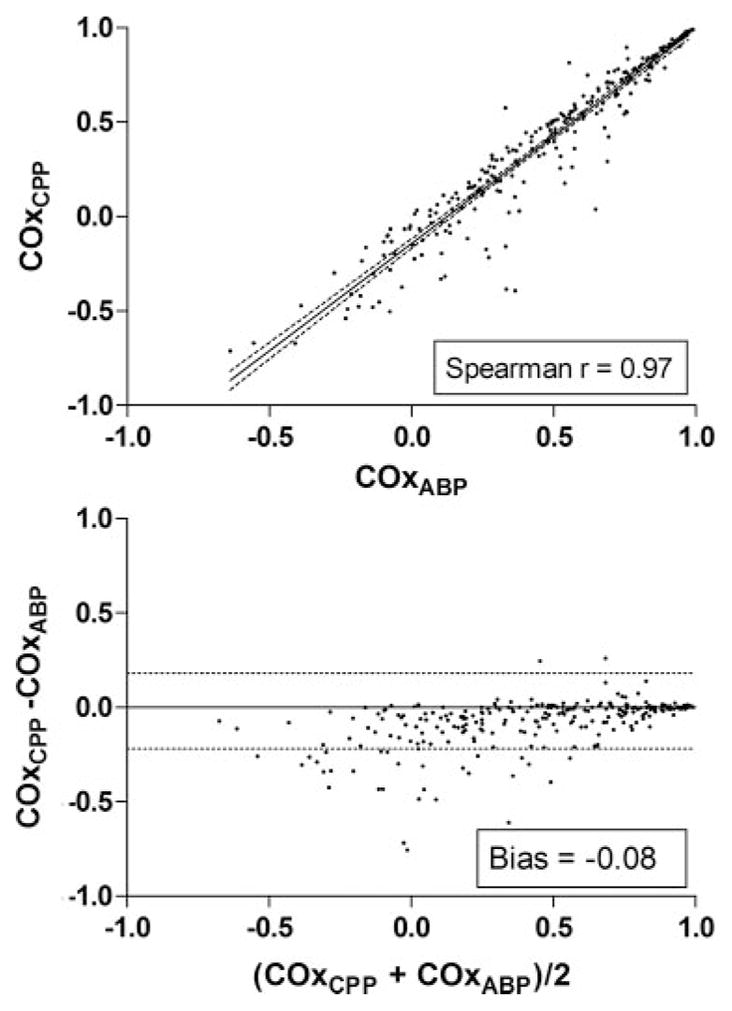
Background: Cerebrovascular autoregulation monitoring is often desirable for critically ill patients in whom intracranial pressure (ICP) is not measured directly. Without ICP, arterial blood pressure (ABP) is a substitute for cerebral perfusion pressure (CPP) to gauge the constraint of cerebral blood flow across pressure changes. We compared the use of ABP versus CPP to measure autoregulation in a piglet model of arterial hypotension.
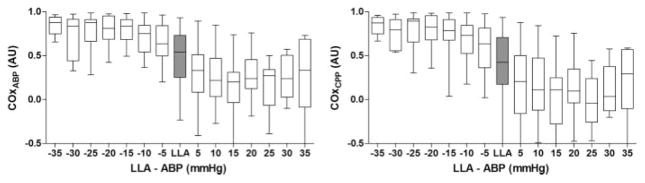
Methods: Our database of neonatal piglet (5-7 days old) experiments was queried for animals with naïve ICP that were made lethally hypotensive to determine the lower limit of autoregulation (LLA). Twenty-five piglets were identified, each with continuous recordings of ICP, regional cerebral oximetry (rSo2), and cortical red cell flux (laser Doppler). Autoregulation was assessed with the cerebral oximetry index (COx) in 2 ways: linear correlation between ABP and rSo2 (COx(ABP)) and between CPP and rSo2 (COx(CPP)). The lower limits of autoregulation were determined from plots of red cell flux versus ABP. Averaged values of COx(ABP) and COx(CPP) from 5 mm Hg ABP bins were used to show receiver operating characteristics for the 2 methods.
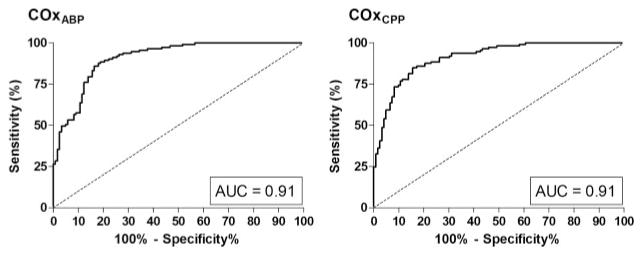
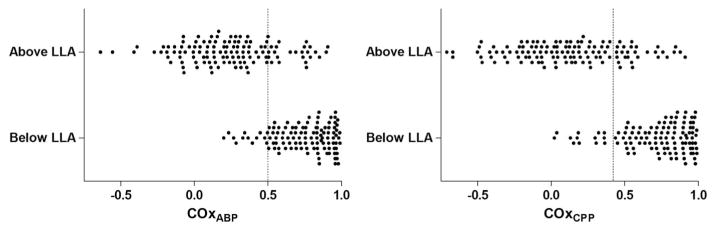
Results: COx(ABP) and COx(CPP) yielded identical receiver operating characteristic curve areas of 0.91 (95% confidence interval [CI], 0.88-0.95) for determining the LLA. However, the thresholds for the 2 methods differed: a threshold COx(ABP) of 0.5 was 89% sensitive (95% CI, 81%-94%) and 81% specific (95% CI, 73%-88%) for detecting ABP below the LLA. A threshold COx(CPP) of 0.42 gave the same 89% sensitivity (95% CI, 81%-94%) with 77% specificity (95% CI, 69%-84%).
Conclusions: The use of ABP instead of CPP for autoregulation monitoring in the naïve brain with COx results in a higher threshold value to discriminate ABP above from ABP below the LLA. However, accuracy was similar with the 2 methods. These findings support and refine the use of near-infrared spectroscopy to monitor autoregulation in patients without ICP monitors.
Figures
Similar articles
-
Validation of Intracranial Pressure-Derived Cerebrovascular Reactivity Indices against the Lower Limit of Autoregulation, Part II: Experimental Model of Arterial Hypotension.J Neurotrauma. 2018 Dec 1;35(23):2812-2819. doi: 10.1089/neu.2017.5604. Epub 2018 Aug 10. J Neurotrauma. 2018. PMID: 29808745 Free PMC article.
-
Validation of Pressure Reactivity and Pulse Amplitude Indices against the Lower Limit of Autoregulation, Part I: Experimental Intracranial Hypertension.J Neurotrauma. 2018 Dec 1;35(23):2803-2811. doi: 10.1089/neu.2017.5603. Epub 2018 Oct 4. J Neurotrauma. 2018. PMID: 29978744 Free PMC article.
-
The lower limit of cerebral blood flow autoregulation is increased with elevated intracranial pressure.Anesth Analg. 2009 Apr;108(4):1278-83. doi: 10.1213/ane.0b013e3181964848. Anesth Analg. 2009. PMID: 19299800
-
Monitoring of cerebrovascular autoregulation: facts, myths, and missing links.Neurocrit Care. 2009;10(3):373-86. doi: 10.1007/s12028-008-9175-7. Epub 2009 Jan 6. Neurocrit Care. 2009. PMID: 19127448 Review.
-
Monitoring of cerebral autoregulation.Neurocrit Care. 2014 Dec;21 Suppl 2:S95-102. doi: 10.1007/s12028-014-0046-0. Neurocrit Care. 2014. PMID: 25208679 Review.
Cited by
-
Individualized perfusion targets in hypoxic ischemic brain injury after cardiac arrest.Crit Care. 2017 Oct 24;21(1):259. doi: 10.1186/s13054-017-1832-9. Crit Care. 2017. PMID: 29061152 Free PMC article. Review.
-
Dopamine therapy does not affect cerebral autoregulation during hypotension in newborn piglets.PLoS One. 2017 Jan 31;12(1):e0170738. doi: 10.1371/journal.pone.0170738. eCollection 2017. PLoS One. 2017. PMID: 28141842 Free PMC article.
-
Cerebral autoregulation after subarachnoid hemorrhage: comparison of three methods.J Cereb Blood Flow Metab. 2013 Mar;33(3):449-56. doi: 10.1038/jcbfm.2012.189. Epub 2012 Dec 12. J Cereb Blood Flow Metab. 2013. PMID: 23232948 Free PMC article. Clinical Trial.
-
[Progress on perioperative monitoring of cerebral blood flow autoregulation].Zhejiang Da Xue Xue Bao Yi Xue Ban. 2015 Jul;44(4):451-7. doi: 10.3785/j.issn.1008-9292.2015.07.16. Zhejiang Da Xue Xue Bao Yi Xue Ban. 2015. PMID: 26555425 Free PMC article. Chinese.
-
Time-Series Autoregressive Models for Point and Interval Forecasting of Raw and Derived Commercial Near-Infrared Spectroscopy Measures: An Exploratory Cranial Trauma and Healthy Control Analysis.Bioengineering (Basel). 2025 Jun 21;12(7):682. doi: 10.3390/bioengineering12070682. Bioengineering (Basel). 2025. PMID: 40722374 Free PMC article.
References
-
- Lassen NA. Cerebral blood flow and oxygen consumption in man. Physiol Rev. 1959;39:183–238. - PubMed
-
- McCall ML. Cerebral circulation and metabolism in toxemia of pregnancy; observations on the effects of veratrum viride and apresoline (1-hydrazinophthalazine) Am J Obstet Gynecol. 1953;66:1015–30. - PubMed
-
- Drummond JC. The lower limit of autoregulation: time to revise our thinking? Anesthesiology. 1997;86:1431–3. - PubMed
-
- Strandgaard S. Autoregulation of cerebral blood flow in hypertensive patients. The modifying influence of prolonged antihypertensive treatment on the tolerance to acute, drug-induced hypotension. Circulation. 1976;53:720–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
