

Can computer-assisted surgery reduce the effective dose for spinal fusion and sacroiliac screw insertion?
- PMID: 20521129
- PMCID: PMC2919865
- DOI: 10.1007/s11999-010-1393-6
Can computer-assisted surgery reduce the effective dose for spinal fusion and sacroiliac screw insertion?
Abstract
Background: The increasing use of fluoroscopy-based surgical procedures and the associated exposure to radiation raise questions regarding potential risks for patients and operating room personnel. Computer-assisted technologies can help to reduce the emission of radiation; the effect on the patient's dose for the three-dimensional (3-D)-based technologies has not yet been evaluated.
Questions/purposes: We determined the effective and organ dose in dorsal spinal fusion and percutaneous transsacral screw stabilization during conventional fluoroscopy-assisted and computer-navigated procedures.
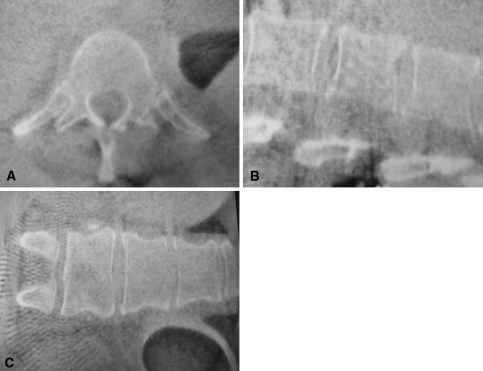
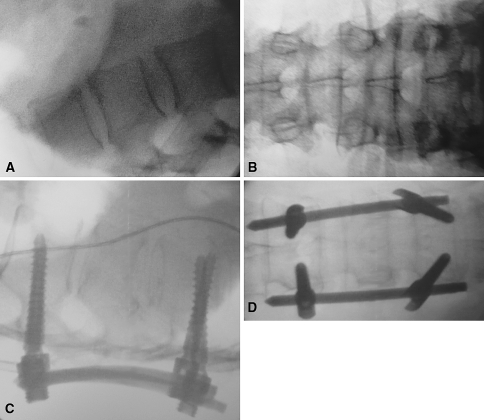
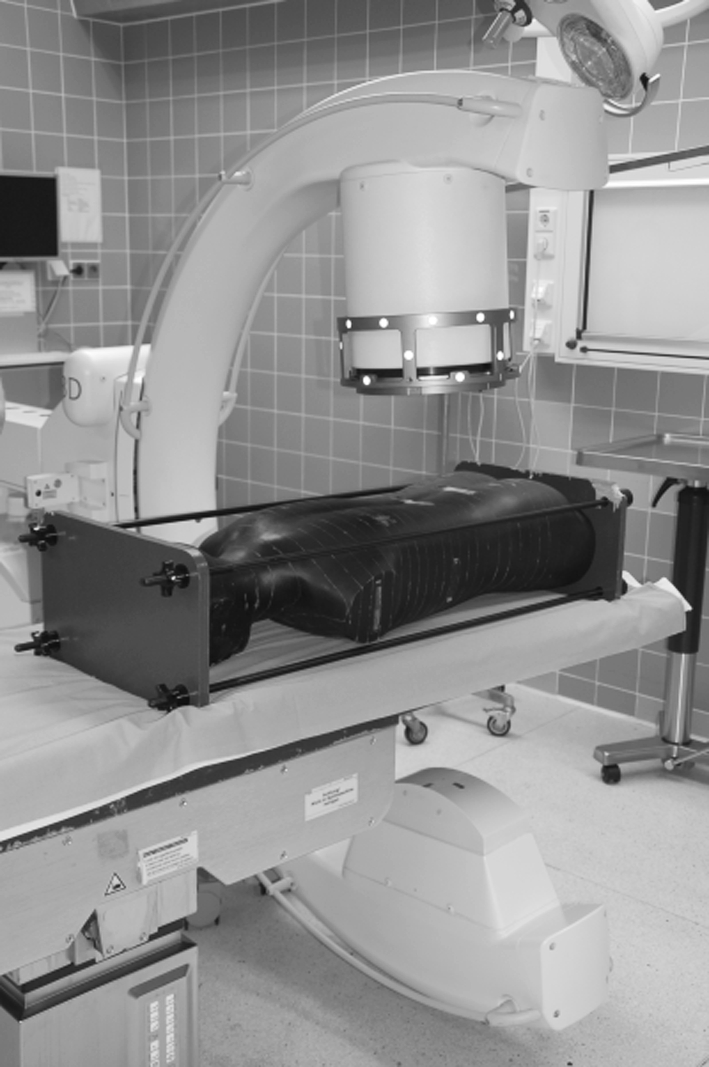
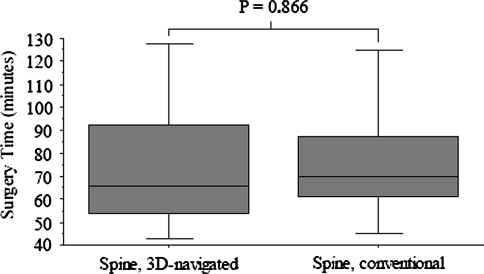
Patients and methods: We recorded the dose and duration of radiation from fluoroscopy in 20 patients, with single vertebra fractures of the lumbar spine, who underwent posterior stabilization with and without the use of a navigation system and 20 patients with navigated percutaneous transsacral screw stabilization for sacroiliac joint injuries. For the conventional iliosacral joint operations, the duration of radiation was estimated retrospectively in two cases and further determined from the literature. Dose measurements were performed with a male phantom; the phantom was equipped with thermoluminescence dosimeters.
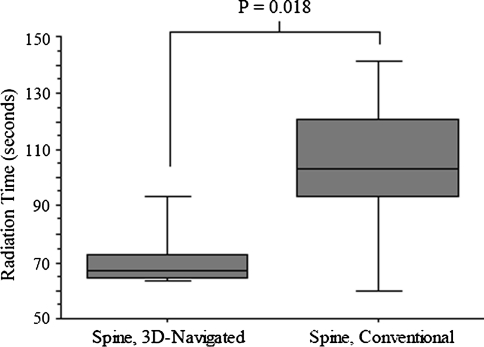
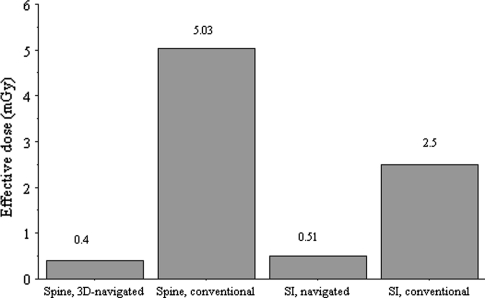
Results: The effective dose in conventional spine surgery using 2-D fluoroscopy was more than 12-fold greater than in navigated operations. For the sacroiliac joint, the effective dose was nearly fivefold greater for nonnavigated operations.
Conclusion: Compared with conventional fluoroscopy, the patient's effective dose can be reduced by 3-D computer-assisted spinal and pelvic surgery.
Level of evidence: Level II, therapeutic study. See Guidelines for Authors for a complete description of levels of evidence.
Figures


References
-
- Carbone JJ, Tortolani PJ, Quartararo LG. Fluoroscopically assisted pedicle screw fixation for thoracic and thoracolumbar injuries: technique and short-term complications. Spine (Phila Pa 1976). 2003;28:91–97. - PubMed
-
- Gaines RW., Jr The use of pedicle-screw internal fixation for the operative treatment of spinal disorders. J Bone Joint Surg Am. 2000;82:1458–1476. - PubMed
-
- Gebhard F, Weidner A, Liener UC, Stockle U, Arand M. Navigation at the spine. Injury. 2004;35(suppl 1):S-A35–45. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
