

Morbidity and mortality associated with the restrictive spirometric pattern: a longitudinal study
- PMID: 20522846
- PMCID: PMC3036842
- DOI: 10.1136/thx.2009.126052
Morbidity and mortality associated with the restrictive spirometric pattern: a longitudinal study
Abstract
Background: Recent studies have suggested that a restrictive pattern assessed with a single spirometric test is associated with increased morbidity and mortality. This study was undertaken to determine demographic, clinical and mortality profiles of subjects with either a recurrent or an inconsistent restrictive spirometric pattern assessed prospectively.
Methods: Data from 2048 adult participants in the population-based TESAOD study were analysed. Normal (forced expiratory volume in 1 s/forced vital capacity (FEV(1)/FVC) ratio >or=70% and FVC >or=80% predicted), restrictive (FEV(1)/FVC >or=70% and FVC <80% predicted) and obstructive (FEV(1)/FVC <70%) patterns were assessed at the enrollment survey in 1972 and in 11 subsequent follow-up surveys up to 1996. Demographic and clinical characteristics were measured at enrollment and vital status and cause of death were assessed at January 2005.
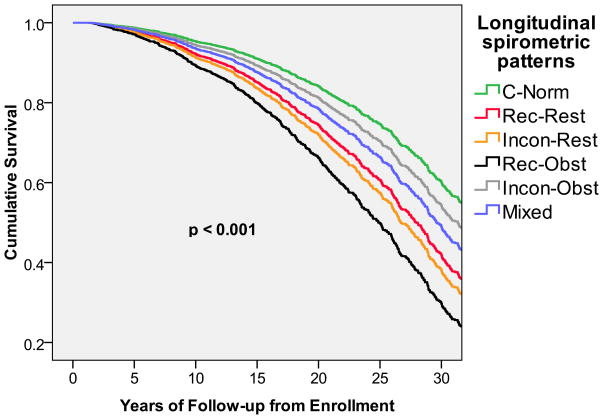
Results: Overall, 12% of participants had a restrictive spirometric pattern at enrollment. They were less likely to be male, to smoke and to have asthma, and had lower IgE levels than subjects in the obstructive group. Among subjects with a restrictive pattern at enrollment, 38% developed an obstructive pattern during follow-up. The remaining 62% had either a recurrent (restrictive pattern >or=50% of follow-up surveys) or inconsistent (restrictive pattern <50% of follow-up surveys) longitudinal restrictive pattern. The recurrent and inconsistent restrictive groups had increased mortality risk for all-cause (adjusted HR 1.7 (95% CI 1.3 to 2.3) and 1.9 (95% CI 1.4 to 2.6), respectively), heart disease (2.0 (95% CI 1.3 to 3.1) and 2.7 (95% CI 1.7 to 4.3)), stroke (2.4 (95% CI 0.9 to 6.3) and 3.5 (95% CI 1.2 to 9.8)) and diabetes (8.0 (95% CI 2.9 to 21.8) and 6.0 (95% CI 1.9 to 19.2)).
Conclusions: The restrictive spirometric pattern identifies a pulmonary condition that is distinguishable from obstructive lung disease and is associated with an increased risk of life-threatening comorbidities.
Conflict of interest statement
None declared.
Figures
Comment in
-
Respiratory disease in 2010: looking to the past will prepare us for the future.Thorax. 2010 Jun;65(6):469-71. doi: 10.1136/thx.2010.137570. Thorax. 2010. PMID: 20522839 No abstract available.
-
Comment on: Morbidity and mortality associated with the restrictive spirometric pattern: a longitudinal study.Thorax. 2011 Sep;66(9):826; author reply 826-7. doi: 10.1136/thx.2010.149419. Epub 2010 Oct 22. Thorax. 2011. PMID: 20971981 No abstract available.
References
-
- Speizer FE, Fay ME, Dockery DW, Ferris BG., Jr Chronic obstructive pulmonary disease mortality in six U.S. cities. Am Rev Respir Dis. 1989;140(3 Pt 2):S49–55. - PubMed
-
- Pauwels RA, Buist AS, Calverley PM, Jenkins CR, Hurd SS. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) Workshop summary. Am J Respir Crit Care Med. 2001;163(5):1256–76. - PubMed
-
- Jemal A, Ward E, Hao Y, Thun M. Trends in the leading causes of death in the United States, 1970–2002. Jama. 2005;294(10):1255–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical