

Anatomical landmarks for safe elevation of the deep inferior epigastric perforator flap: a cadaveric study
- PMID: 20523907
- PMCID: PMC2878755
Anatomical landmarks for safe elevation of the deep inferior epigastric perforator flap: a cadaveric study
Abstract
Background: Breast reconstruction techniques have focused increasingly on using autologous tissue, with emphasis being placed on employing muscle sparing adipocutaneous flaps to reduce abdominal wall complications such as hernias, bulges, weakness, and length of hospital stay. The result has been the emergence of the deep inferior epigastric perforator (DIEP) flap for breast reconstruction. Isolating perforator vessels challenges most surgeons. We describe surface anatomical landmarks to predict the location of the deep inferior epigastric artery (DIEA) and its perforators to aid in the efficient elevation of this flap.
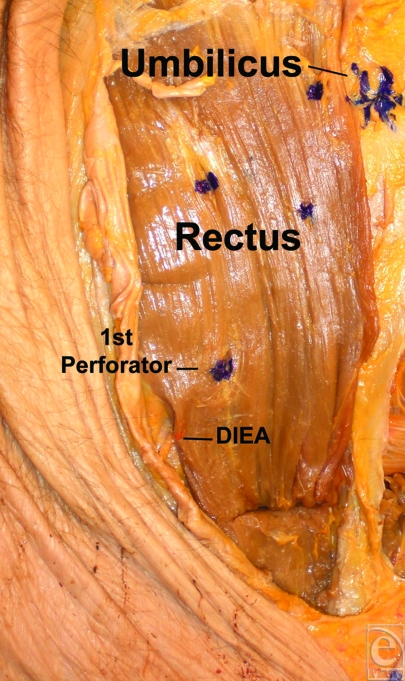
Methods: Ten fresh hemi-abdomens were dissected with loupe magnification. The DIEA and its perforators were identified, and measurements in relation to the rectus muscle, xiphoid, umbilicus, and pubis were taken. Statistical analysis was undertaken to determine distance ratios to account for variance in patient size.
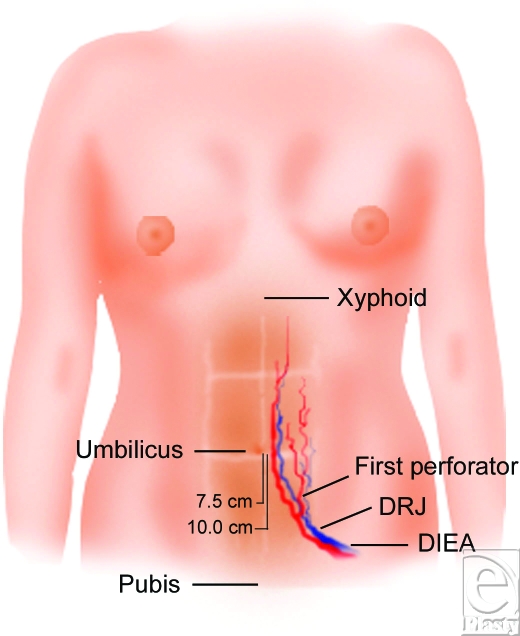
Results: Average distance from the xiphoid to umbilicus was 18.2 +/- 1.27 cm. The distance from the umbilicus to pubis was 14.9 +/- 2.3 cm. The vertical distance from the umbilicus to the DRJ (DIEA rtctus junction) was 10.45 +/- 1.58 cm, and the vertical distance from the level of the umbilicus to where the first DIEA perforator traverses the RAM was 7.4 +/- 1.64 cm. The distance between the umbilicus and the DRJ is approximately 0.7 times the distance between the umbilicus and the pubic symphysis. The distance between the umbilicus and the first perforator is approximately 0.5 times the distance between the umbilicus and the pubic symphysis.
Conclusions: Knowledge of anatomical landmarks can aid the surgeon in more efficiently harvesting the DIEP flap. Surface landmarks along the abdominal midline coupled with normalizing ratios can aid surgeons in predicting the location of the DIEA and its first perforator. The DIEA crosses the rectus at approximately two thirds of the distance between the umbilicus and pubis, and the first perforator can reliably be located at one half of this distance.
Figures

References
-
- Rozen W-M, Ashton M-W, Pan WR, Taylor GI. Raising perforator flaps for breast reconstruction: the intramuscular anatomy of the DIEA. Plast Reconstr Surg. 2007;120:1443–9. - PubMed
-
- Nano M-T, Gill P-G, Kollias J, Bochner MA, Carter N, Winefield HR. Qualitative assessment of breast reconstruction in a specialist breast unit. Aust N Z J Surg. 2005;75:445–3. - PubMed
-
- Allen R-J. DIEP versus TRAM for breast reconstruction. Plast Reconstr Surg. 2003;111:466–75. - PubMed
-
- Chen M-C, Halvorson E-G, Disa JJ, et al. Immediate postoperative complications in DIEP versus free/muscle-sparing TRAM flaps. Plast Reconstr Surg. 2007;120:1477–82. - PubMed
-
- Kroll S-S, Sharma S, Koutz C, et al. Postoperative morphine requirements of free TRAM and DIEP flaps. Plast Reconstr Surg. 2001;107:338–41. - PubMed
LinkOut - more resources
Full Text Sources