

Factors involved in maintaining prolonged functional independence following supratentorial glioblastoma resection. Clinical article
- PMID: 20524825
- PMCID: PMC3725949
- DOI: 10.3171/2010.4.JNS091340
Factors involved in maintaining prolonged functional independence following supratentorial glioblastoma resection. Clinical article
Abstract
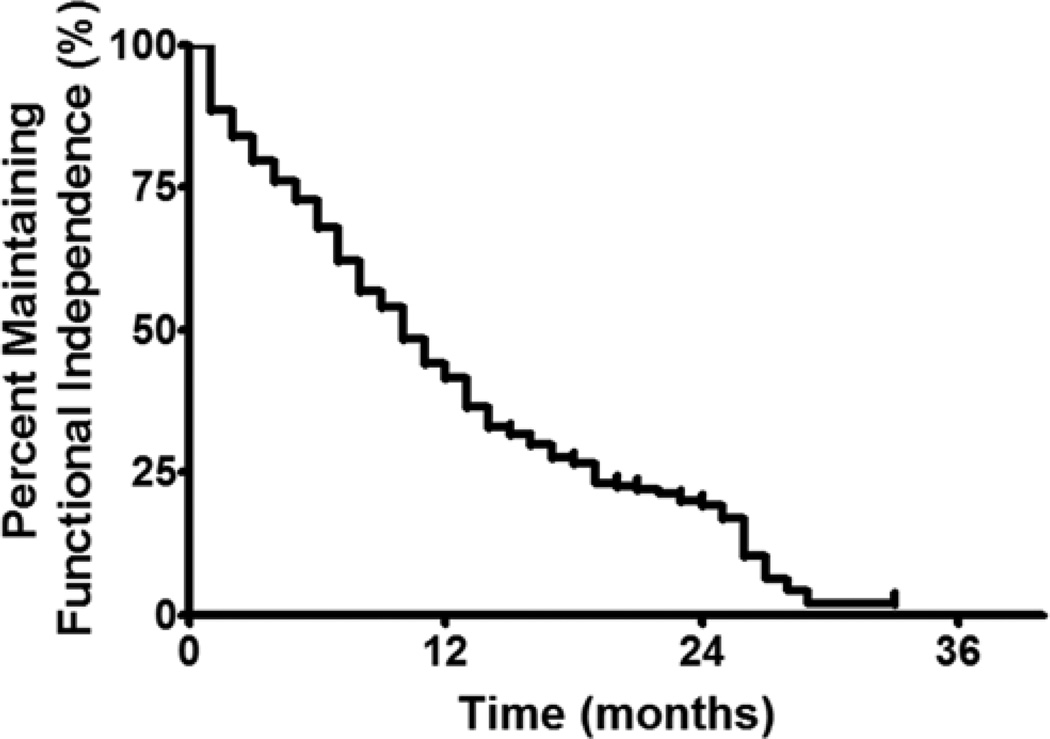
Object: The median survival duration for patients with glioblastoma is approximately 12 months. Maximizing quality of life (QOL) for patients with glioblastoma is a priority. An important, yet understudied, QOL component is functional independence. The aims of this study were to evaluate functional outcomes over time for patients with glioblastoma, as well as identify factors associated with prolonged functional independence.
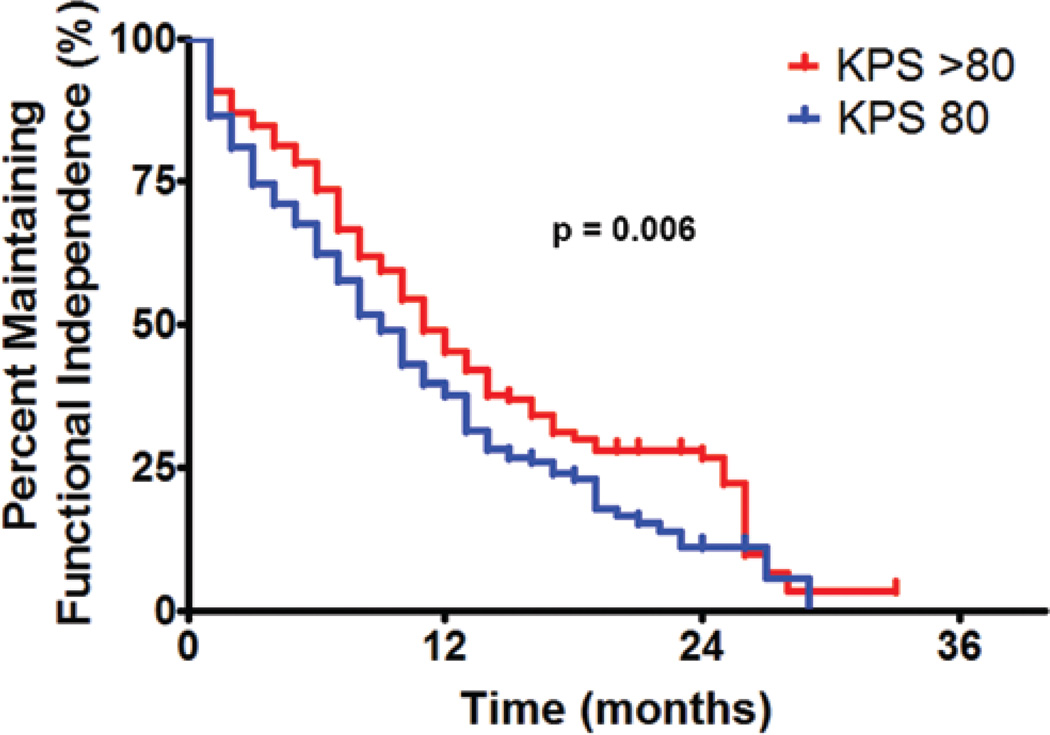
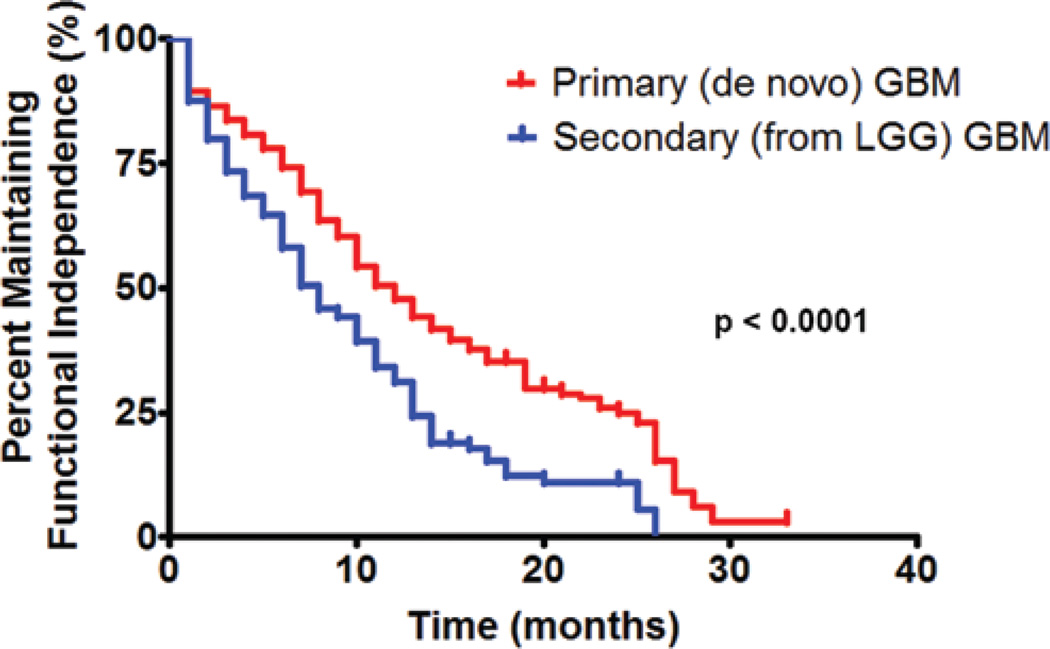
Methods: All patients who underwent first-time resection of either a primary (de novo) or secondary (prior lower grade glioma) glioblastoma at a single institution from 1996 to 2006 were retrospectively reviewed. Patients with a Karnofsky Performance Scale (KPS) score ≥ 80 were included. Kaplan-Meier, log-rank, and multivariate proportional hazards regression analyses were used to identify associations (p < 0.05) with functional independence (KPS score ≥ 60) following glioblastoma resection.
Results: The median follow-up duration time was 10 months (interquartile range [IQR] 5.6-17.0 months). A patient's preoperative (p = 0.02) and immediate postoperative (within 2 months) functional status was associated with prolonged survival (p < 0.0001). Of the 544 patients in this series, 302 (56%) lost their functional independence at a median of 10 months (IQR 6-16 months). Factors independently associated with prolonged functional independence were: preoperative KPS score ≥ 90 (p = 0.004), preoperative seizures (p = 0.002), primary glioblastoma (p < 0.0001), gross-total resection (p < 0.0001), and temozolomide chemotherapy (p < 0.0001). Factors independently associated with decreased functional independence were: older age (p < 0.0001), coexistent coronary artery disease (p = 0.009), and incurring a new postoperative motor deficit (p = 0.009). Furthermore, a decline in functional status was independently associated with tumor recurrence (p = 0.01).
Conclusions: The identification and consideration of these factors associated with prolonged functional outcome (preoperative KPS score ≥ 90, seizures, primary glioblastoma, gross-total resection, temozolomide) and decreased functional outcome (older age, coronary artery disease, new postoperative motor deficit) may help guide treatment strategies aimed at improving QOL for patients with glioblastoma.
Conflict of interest statement
The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.
Figures
References
-
- al-Sarraj S, Bridges LR. p53 immunoreactivity in astrocytomas and its relationship to survival. Br J Neurosurg. 1995;9:143–149. - PubMed
-
- Altman DG. Practical Statistics for Medical Research. New York: Chapman & Hall/CRC; 1991.
-
- Barker FG, II, Prados MD, Chang SM, Gutin PH, Lamborn KR, Larson DA, et al. Radiation response and survival time in patients with glioblastoma multiforme. J Neurosurg. 1996;84:442–448. - PubMed
-
- Boarini DJ, Beck DW, VanGilder JC. Postoperative prophylactic anticonvulsant therapy in cerebral gliomas. Neurosurgery. 1985;16:290–292. - PubMed
-
- Brown PD, Ballman KV, Rummans TA, Maurer MJ, Sloan JA, Boeve BF, et al. Prospective study of quality of life in adults with newly diagnosed high-grade gliomas. J Neurooncol. 2006;76:283–291. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
