

The physical basis of ventilator-induced lung injury
- PMID: 20524920
- PMCID: PMC2904955
- DOI: 10.1586/ers.10.28
The physical basis of ventilator-induced lung injury
Abstract
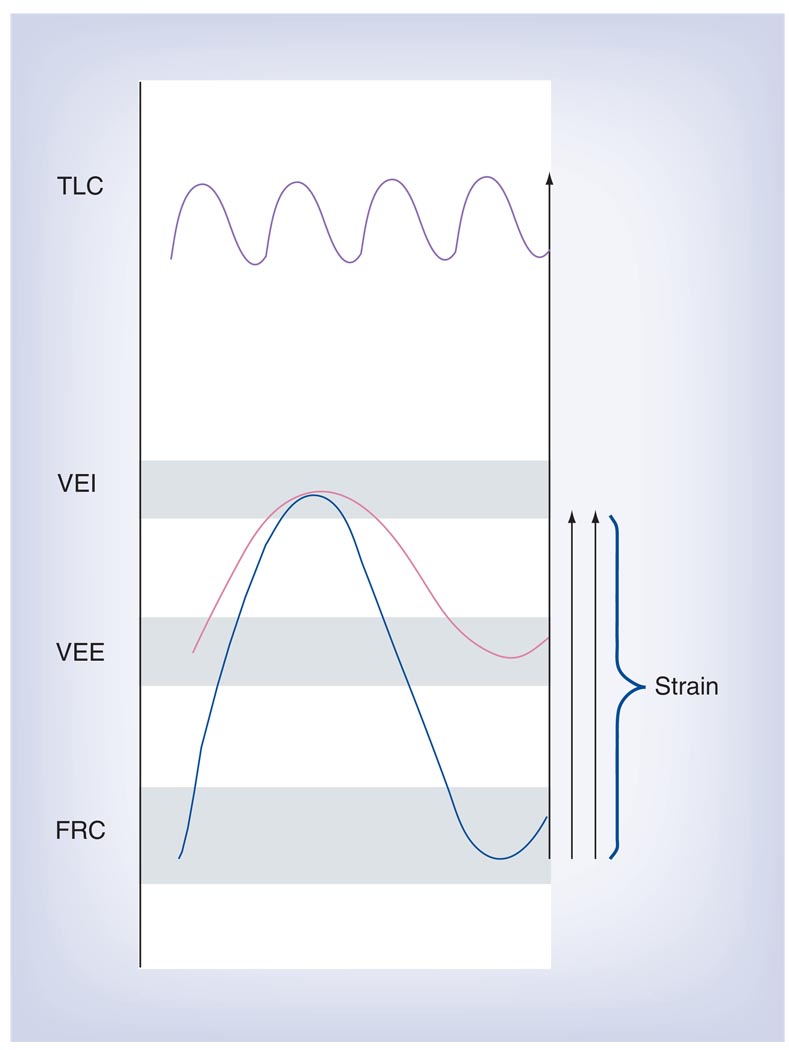
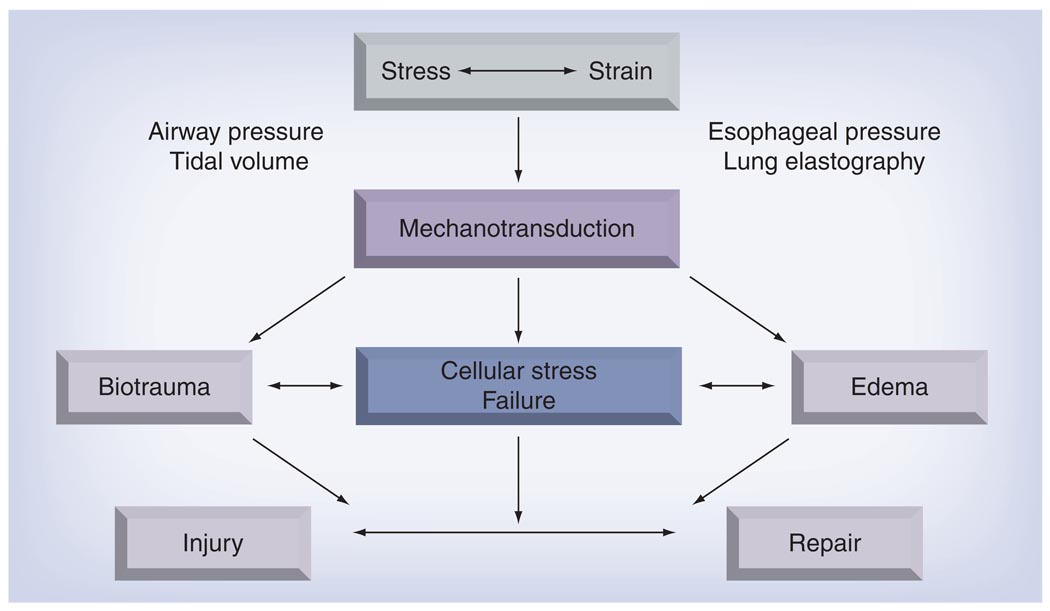
Although mechanical ventilation (MV) is a life-saving intervention for patients with acute respiratory distress syndrome (ARDS), it can aggravate or cause lung injury, known as ventilator-induced lung injury (VILI). The biophysical characteristics of heterogeneously injured ARDS lungs increase the parenchymal stress associated with breathing, which is further aggravated by MV. Cells, in particular those lining the capillaries, airways and alveoli, transform this strain into chemical signals (mechanotransduction). The interaction of reparative and injurious mechanotransductive pathways leads to VILI. Several attempts have been made to identify clinical surrogate measures of lung stress/strain (e.g., density changes in chest computed tomography, lower and upper inflection points of the pressure-volume curve, plateau pressure and inflammatory cytokine levels) that could be used to titrate MV. However, uncertainty about the topographical distribution of stress relative to that of the susceptibility of the cells and tissues to injury makes the existence of a single 'global' stress/strain injury threshold doubtful.
Figures
References
-
- Bernard GR, Artigas A, Brigham KL, et al. The American–European Consensus Conference on ARDS. Definitions, mechanisms, relevant outcomes, and clinical trial coordination. Am. J. Respir. Crit. Care Med. 1994;149(3 Pt 1):818–824. - PubMed
-
-
Ashbaugh DG, Bigelow DB, Petty TL, Levine BE. Acute respiratory distress in adults. Lancet. 1967;2(7511):319–323. • The first description of 12 adult patients with acute respiratory distress syndrome (ARDS).
-
-
-
Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. The Acute Respiratory Distress Syndrome Network. N. Engl. J. Med. 2000;342(18):1301–1308. •• ARDS Network study demonstrating benefit by comparing mortality with a tidal volume of 6 versus 12 ml/kg predicted bodyweight in patients with ARDS.
-
-
- Brower RG, Lanken PN, MacIntyre N, et al. Higher versus lower positive end-expiratory pressures in patients with the acute respiratory distress syndrome. N. Engl. J. Med. 2004;351(4):327–336. - PubMed
-
- Steinberg KP, Hudson LD, Goodman RB, et al. Efficacy and safety of corticosteroids for persistent acute respiratory distress syndrome. N. Engl. J. Med. 2006;354(16):1671–1684. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources