

Cerebrospinal fluid neopterin: an informative biomarker of central nervous system immune activation in HIV-1 infection
- PMID: 20525234
- PMCID: PMC2890504
- DOI: 10.1186/1742-6405-7-15
Cerebrospinal fluid neopterin: an informative biomarker of central nervous system immune activation in HIV-1 infection
Abstract
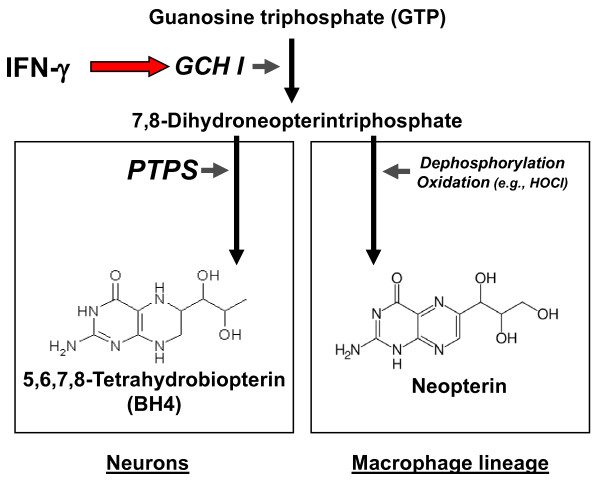
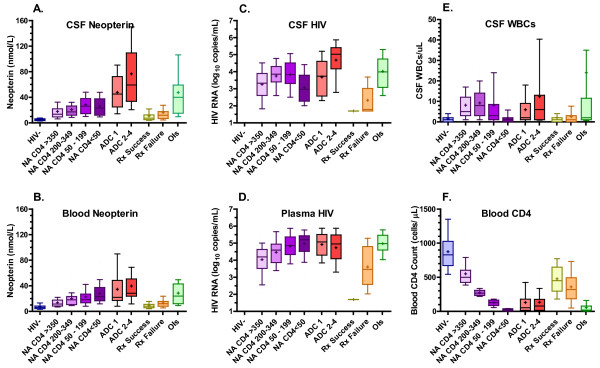
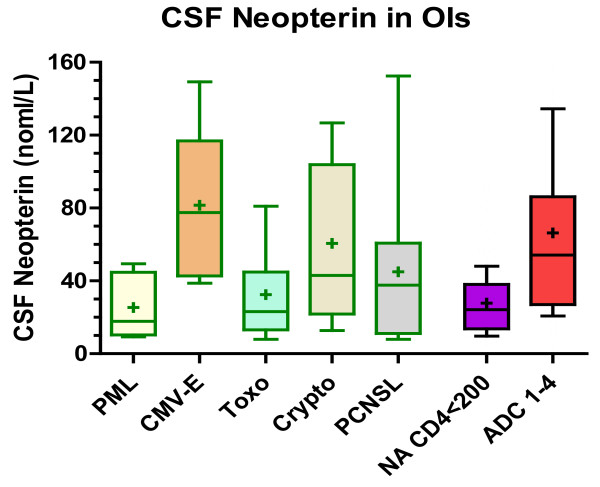
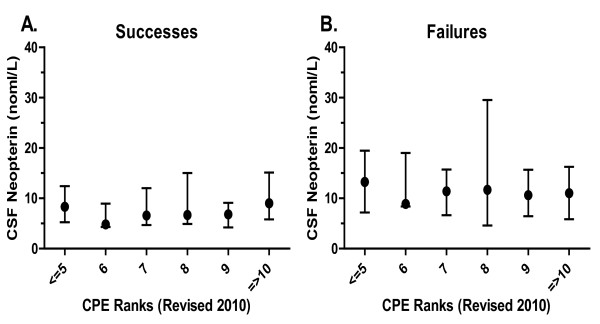
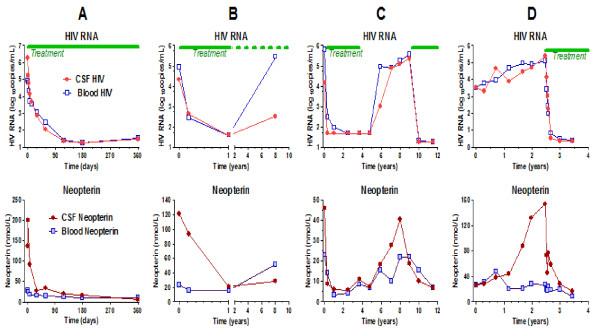
HIV-1 invades the central nervous system (CNS) in the context of acute infection, persists thereafter in the absence of treatment, and leads to chronic intrathecal immunoactivation that can be measured by the macrophage activation marker, neopterin, in cerebrospinal fluid (CSF). In this review we describe our experience with CSF neopterin measurements in 382 untreated HIV-infected patients across the spectrum of immunosuppression and HIV-related neurological diseases, in 73 untreated AIDS patients with opportunistic CNS infections, and in 233 treated patients.In untreated patients, CSF neopterin concentrations are almost always elevated and increase progressively as immunosuppression worsens and blood CD4 cell counts fall. However, patients with HIV dementia exhibit particularly high CSF neopterin concentrations, above those of patients without neurological disease, though patients with CNS opportunistic infections, including CMV encephalitis and cryptococcal meningitis, also exhibit high levels of CSF neopterin. Combination antiretroviral therapy, with its potent effect on CNS HIV infection and CSF HIV RNA, mitigates both intrathecal immunoactivation and lowers CSF neopterin. However, despite suppression of plasma and CSF HIV RNA to below the detection limits of clinical assays (<50 copies HIV RNA/mL), CSF neopterin often remains mildly elevated, indicating persistent low-level intrathecal immune activation and raising the important questions of whether this elevation is driven by continued CNS infection and whether it causes continued indolent CNS injury.Although nonspecific, CSF neopterin can serve as a useful biomarker in the diagnosis of HIV dementia in the setting of confounding conditions, in monitoring the CNS inflammatory effects of antiretroviral treatment, and give valuable information to the cause of ongoing brain injury.
Figures
Similar articles
-
Low levels of HIV-1 RNA detected in the cerebrospinal fluid after up to 10 years of suppressive therapy are associated with local immune activation.AIDS. 2014 Sep 24;28(15):2251-8. doi: 10.1097/QAD.0000000000000400. AIDS. 2014. PMID: 25022595 Free PMC article.
-
Persistent intrathecal immune activation in HIV-1-infected individuals on antiretroviral therapy.J Acquir Immune Defic Syndr. 2008 Feb 1;47(2):168-73. doi: 10.1097/QAI.0b013e31815ace97. J Acquir Immune Defic Syndr. 2008. PMID: 17971711 Free PMC article.
-
Cerebrospinal fluid HIV-1 RNA, intrathecal immunoactivation, and drug concentrations after treatment with a combination of saquinavir, nelfinavir, and two nucleoside analogues: the M61022 study.BMC Infect Dis. 2006 Mar 27;6:63. doi: 10.1186/1471-2334-6-63. BMC Infect Dis. 2006. PMID: 16566834 Free PMC article.
-
Antiretroviral treatment of central nervous system HIV-1 infection: a review.HIV Med. 2001 Apr;2(2):97-104. doi: 10.1046/j.1468-1293.2001.00056.x. HIV Med. 2001. PMID: 11737386 Review.
-
Defining and evaluating HIV-related neurodegenerative disease and its treatment targets: a combinatorial approach to use of cerebrospinal fluid molecular biomarkers.J Neuroimmune Pharmacol. 2007 Mar;2(1):112-9. doi: 10.1007/s11481-006-9035-1. Epub 2006 Sep 12. J Neuroimmune Pharmacol. 2007. PMID: 18040834 Review.
Cited by
-
No support for premature central nervous system aging in HIV-1 when measured by cerebrospinal fluid phosphorylated tau (p-tau).Virulence. 2017 Jul 4;8(5):599-604. doi: 10.1080/21505594.2016.1212155. Epub 2016 Jul 19. Virulence. 2017. PMID: 27435879 Free PMC article.
-
Compartmentalization of cerebrospinal fluid inflammation across the spectrum of untreated HIV-1 infection, central nervous system injury and viral suppression.PLoS One. 2021 May 13;16(5):e0250987. doi: 10.1371/journal.pone.0250987. eCollection 2021. PLoS One. 2021. PMID: 33983973 Free PMC article.
-
Cerebrospinal fluid concentrations of tenofovir and emtricitabine in the setting of HIV-1 protease inhibitor-based regimens.J Clin Pharmacol. 2016 Apr;56(4):492-6. doi: 10.1002/jcph.612. Epub 2015 Oct 20. J Clin Pharmacol. 2016. PMID: 26247878 Free PMC article. No abstract available.
-
Cerebrospinal fluid biomarkers in SARS-CoV-2 patients with acute neurological syndromes.Rev Neurol (Paris). 2023 Mar;179(3):208-217. doi: 10.1016/j.neurol.2022.11.002. Epub 2022 Nov 30. Rev Neurol (Paris). 2023. PMID: 36610823 Free PMC article.
-
Optimal treatment of HIV-associated neurocognitive disorders: myths and reality. A critical review.Ther Adv Infect Dis. 2019 Apr 4;6:2049936119838228. doi: 10.1177/2049936119838228. eCollection 2019 Jan-Dec. Ther Adv Infect Dis. 2019. PMID: 31001421 Free PMC article. Review.
References
-
- Fuchs D, Spira TJ, Hausen A, Reibnegger G, Werner ER, Felmayer GW, Wachter H. Neopterin as a predictive marker for disease progression in human immunodeficiency virus type 1 infection. Clin Chem. 1989;35(8):1746–1749. - PubMed
-
- Fuchs D, Chiodi F, Albert J, Asjo B, Hagberg L, Hausen A, Norkrans G, Reibnegger G, Werner ER, Wachter H. Neopterin concentrations in cerebrospinal fluid and serum of individuals infected with HIV-1. AIDS (London, England) 1989;3(5):285–288. - PubMed
-
- Sonnerborg AB, von Stedingk LV, Hansson LO, Strannegard OO. Elevated neopterin and beta 2-microglobulin levels in blood and cerebrospinal fluid occur early in HIV-1 infection. AIDS (London, England) 1989;3(5):277–283. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
