

Depression diagnoses following the identification of bipolar disorder: costly incongruent diagnoses
- PMID: 20525372
- PMCID: PMC2894758
- DOI: 10.1186/1471-244X-10-39
Depression diagnoses following the identification of bipolar disorder: costly incongruent diagnoses
Abstract
Background: Previous research has documented that the symptoms of bipolar disorder are often mistaken for unipolar depression prior to a patient's first bipolar diagnosis. The assumption has been that once a patient receives a bipolar diagnosis they will no longer be given a misdiagnosis of depression. The objectives of this study were 1) to assess the rate of subsequent unipolar depression diagnosis in individuals with a history of bipolar disorder and 2) to assess the increased cost associated with this potential misdiagnosis.
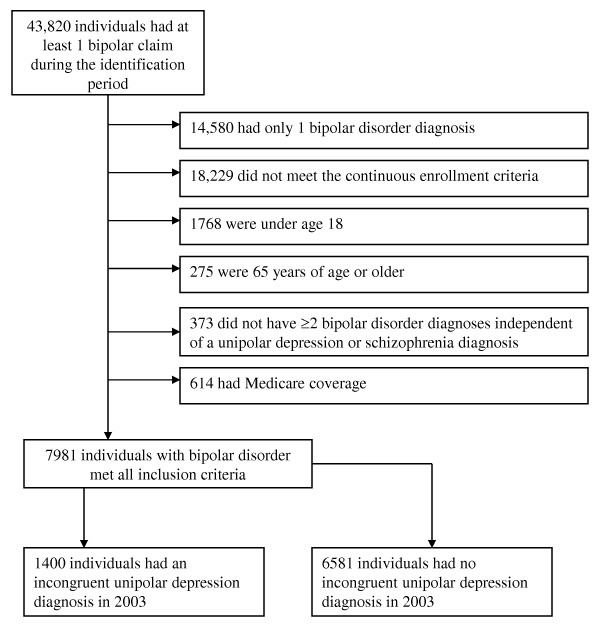
Methods: This study utilized a retrospective cohort design using administrative claims data from 2002 and 2003. Patient inclusion criteria for the study were 1) at least 2 bipolar diagnoses in 2002, 2) continuous enrollment during 2002 and 2003, 3) a pharmacy benefit, and 4) age 18 to 64. Patients with at least 2 unipolar depression diagnoses in 2003 were categorized as having an incongruent diagnosis of unipolar depression. We used propensity scoring to control for selection bias. Utilization was evaluated using negative binomial models. We evaluated cost differences between patient cohorts using generalized linear models.
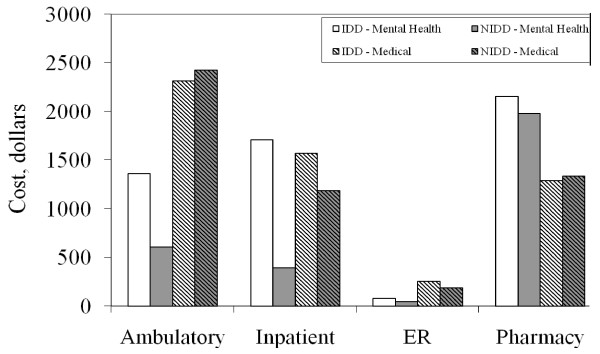
Results: Of the 7981 patients who met all inclusion criteria for the analysis, 17.5% (1400) had an incongruent depression diagnosis (IDD). After controlling for background differences, individuals who received an IDD had higher rates of inpatient and outpatient psychiatric utilization and cost, on average, an additional $1641 per year compared to individuals without an IDD.
Conclusions: A strikingly high proportion of bipolar patients are given the differential diagnosis of unipolar depression after being identified as having bipolar disorder. Individuals with an IDD had increased acute psychiatric care services, suggesting higher levels of relapses, and were at risk for inappropriate treatment, as antidepressant therapy without a concomitant mood-stabilizing medication is contraindicated in bipolar disorder. Further prospective research is needed to validate the findings from this retrospective administrative claims-based analysis.
Figures
Similar articles
-
Diagnosis of unipolar depression following initial identification of bipolar disorder: a common and costly misdiagnosis.J Clin Psychiatry. 2008 May;69(5):749-58. doi: 10.4088/jcp.v69n0508. J Clin Psychiatry. 2008. PMID: 18363423
-
Misdiagnosed patients with bipolar disorder: comorbidities, treatment patterns, and direct treatment costs.J Clin Psychiatry. 2005 Nov;66(11):1432-40. doi: 10.4088/jcp.v66n1114. J Clin Psychiatry. 2005. PMID: 16420081
-
Service utilization and associated direct costs for bipolar disorder in 2004: an analysis in managed care.J Affect Disord. 2007 Aug;101(1-3):187-93. doi: 10.1016/j.jad.2006.11.019. Epub 2007 Jan 23. J Affect Disord. 2007. PMID: 17254637
-
Clinical and economic effects of unrecognized or inadequately treated bipolar disorder.J Psychiatr Pract. 2008 May;14 Suppl 2:31-8. doi: 10.1097/01.pra.0000320124.91799.2a. J Psychiatr Pract. 2008. PMID: 18677197 Review.
-
Strategies to reduce misdiagnosis of bipolar depression.Psychiatr Serv. 2001 Jan;52(1):51-5. doi: 10.1176/appi.ps.52.1.51. Psychiatr Serv. 2001. PMID: 11141528 Review.
Cited by
-
The Economic Burden of Bipolar Disorder in the United States: A Systematic Literature Review.Clinicoecon Outcomes Res. 2020 Sep 7;12:481-497. doi: 10.2147/CEOR.S259338. eCollection 2020. Clinicoecon Outcomes Res. 2020. PMID: 32982338 Free PMC article. Review.
-
Glia and immune cell signaling in bipolar disorder: insights from neuropharmacology and molecular imaging to clinical application.Transl Psychiatry. 2014 Jan 21;4(1):e350. doi: 10.1038/tp.2013.119. Transl Psychiatry. 2014. PMID: 24448212 Free PMC article. Review.
-
Validity of the 32-item Hypomania Checklist (HCL-32) in a clinical sample with mood disorders in China.BMC Psychiatry. 2011 May 15;11:84. doi: 10.1186/1471-244X-11-84. BMC Psychiatry. 2011. PMID: 21575151 Free PMC article. Clinical Trial.
-
Anterior cingulate cortex choline levels in female adolescents with unipolar versus bipolar depression: a potential new tool for diagnosis.J Affect Disord. 2014;167:25-9. doi: 10.1016/j.jad.2014.05.051. Epub 2014 Jun 2. J Affect Disord. 2014. PMID: 25082110 Free PMC article.
-
Within- and Between-Session Changes in Neural Activity During Emotion Processing in Unipolar and Bipolar Depression.Biol Psychiatry Cogn Neurosci Neuroimaging. 2016 Nov;1(6):518-527. doi: 10.1016/j.bpsc.2016.03.005. Biol Psychiatry Cogn Neurosci Neuroimaging. 2016. PMID: 28083566 Free PMC article.
References
-
- Kessler RC, McGonagle KA, Zhao S, Nelson CB, Hughes M, Eshleman S, Wittchen HU, Kendler KS. Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States. Results from the National Comorbidity Survey. Arch Gen Psychiatry. 1994;51:8–19. - PubMed
-
- Weissman MM, Bland RC, Canino GJ, Faravelli C, Greenwald S, Hwu HG, Joyce PR, Karam EG, Lee CK, Lellouch J, Lépine JP, Newman SC, Rubio-Stipec M, Wells JE, Wickramaratne PJ, Wittchen H, Yeh EK. Cross-national epidemiology of major depression and bipolar disorder. JAMA. 1996;276:293–299. doi: 10.1001/jama.276.4.293. - DOI - PubMed
-
- Unutzer J, Simon G, Pabiniak C, Bond K, Katon W. The treated prevalence of bipolar disorder in a large staff-model HMO. Psychiatr Serv. 1998;49:1072–1078. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
