

Prohormones for prediction of adverse medical outcome in community-acquired pneumonia and lower respiratory tract infections
- PMID: 20529344
- PMCID: PMC2911752
- DOI: 10.1186/cc9055
Prohormones for prediction of adverse medical outcome in community-acquired pneumonia and lower respiratory tract infections
Abstract
Introduction: Measurement of prohormones representing different pathophysiological pathways could enhance risk stratification in patients with community-acquired pneumonia (CAP) and other lower respiratory tract infections (LRTI).
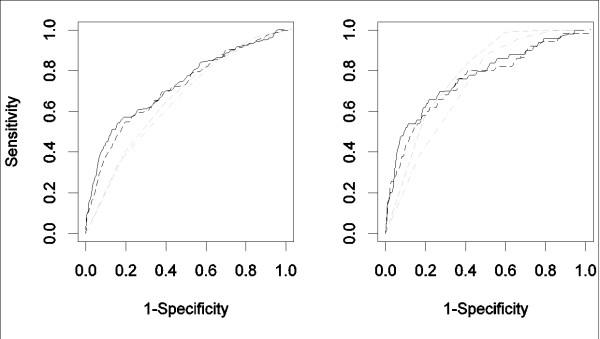
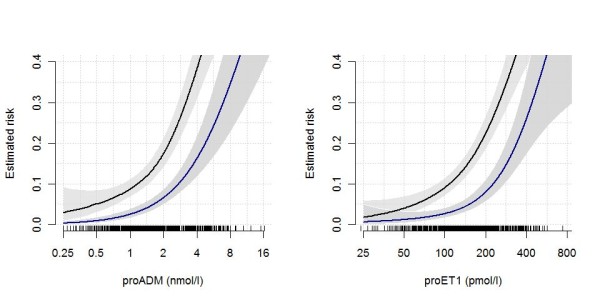
Methods: We assessed clinical parameters and five biomarkers, the precursor levels of adrenomedullin (ADM), endothelin-1 (ET1), atrial-natriuretic peptide (ANP), anti-diuretic hormone (copeptin), and procalcitonin in patients with LRTI and CAP enrolled in the multicenter ProHOSP study. We compared the prognostic accuracy of these biomarkers with the pneumonia severity index (PSI) and CURB65 (Confusion, Urea, Respiratory rate, Blood pressure, Age 65) score to predict serious complications defined as death, ICU admission and disease-specific complications using receiver operating curves (ROC) and reclassification methods.
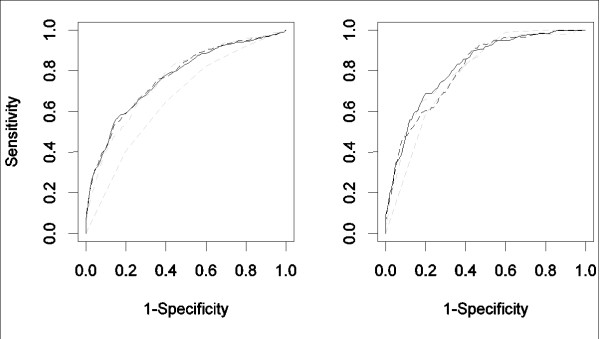
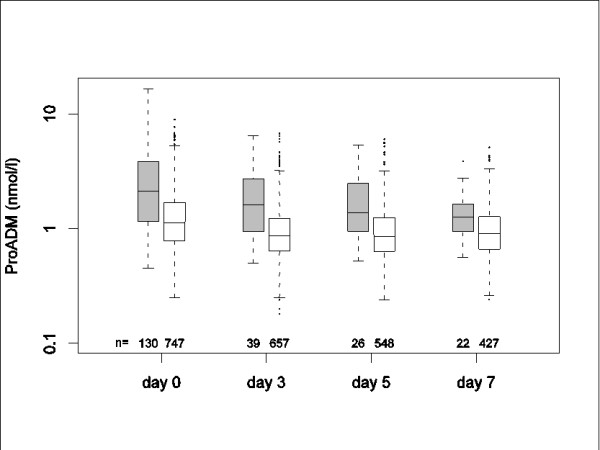
Results: During the 30 days of follow-up, 134 serious complications occurred in 925 (14.5%) patients with CAP. Both PSI and CURB65 overestimated the observed mortality (X2 goodness of fit test: P = 0.003 and 0.01). ProADM or proET1 alone had stronger discriminatory powers than the PSI or CURB65 score or any of either score components to predict serious complications. Adding proADM alone (or all five biomarkers jointly) to the PSI and CURB65 scores, significantly increased the area under the curve (AUC) for PSI from 0.69 to 0.75, and for CURB65 from 0.66 to 0.73 (P < 0.001, for both scores). Reclassification methods also established highly significant improvement (P < 0.001) for models with biomarkers if clinical covariates were more flexibly adjusted for. The developed prediction models with biomarkers extrapolated well if evaluated in 434 patients with non-CAP LRTIs.
Conclusions: Five biomarkers from distinct biologic pathways were strong and specific predictors for short-term adverse outcome and improved clinical risk scores in CAP and non-pneumonic LRTI. Intervention studies are warranted to show whether an improved risk prognostication with biomarkers translates into a better clinical management and superior allocation of health care resources.
Trial registration: NCT00350987.
Figures
References
-
- Niederman MS, Mandell LA, Anzueto A, Bass JB, Broughton WA, Campbell GD, Dean N, File T, Fine MJ, Gross PA, Martinez F, Marrie TJ, Plouffe JF, Ramirez J, Sarosi GA, Torres A, Wilson R, Yu VL. Guidelines for the management of adults with community-acquired pneumonia. Diagnosis, assessment of severity, antimicrobial therapy, and prevention. Am J Respir Crit Care Med. 2001;163:1730–1754. - PubMed
-
- Mandell LA, Wunderink RG, Anzueto A, Bartlett JG, Campbell GD, Dean NC, Dowell SF, File TM Jr, Musher DM, Niederman MS, Torres A, Whitney CG. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007;44(Suppl 2):S27–72. doi: 10.1086/511159. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
