

Accuracy of symptoms and signs for coronary heart disease assessed in primary care
- PMID: 20529488
- PMCID: PMC2880766
- DOI: 10.3399/bjgp10X502137
Accuracy of symptoms and signs for coronary heart disease assessed in primary care
Abstract
Background: Diagnosing the aetiology of chest pain is challenging. There is still a lack of data on the diagnostic accuracy of signs and symptoms for acute coronary events in low-prevalence settings.
Aim: To evaluate the diagnostic accuracy of symptoms and signs in patients presenting to general practice with chest pain.
Design of study: Cross-sectional diagnostic study with delayed-type reference standard.
Setting: Seventy-four general practices in Germany.
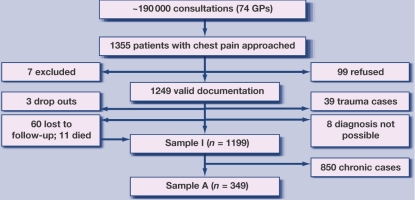
Method: The study included 1249 consecutive patients presenting with chest pain. Data were reviewed by an independent reference panel, with coronary heart disease (CHD) and an indication for urgent hospital admission as reference conditions. Main outcome measures were sensitivity, specificity, likelihood ratio, predictive value, and odds ratio (OR) for non-trauma patients with a reference diagnosis.
Results: Several signs and symptoms showed strong associations with CHD, including known vascular disease (OR = 5.13; 95% confidence interval [CI] = 2.83 to 9.30), pain worse on exercise (OR = 4.27; 95% CI = 2.31 to 7.88), patient assumes cardiac origin of pain (OR = 3.20; 95% CI = 1.53 to 6.60), cough present (OR = 0.08; 95% CI = 0.01 to 0.77), and pain reproducible on palpation (OR = 0.27; 95% CI = 0.13 to 0.56). For urgent hospital admission, effective criteria included pain radiating to the left arm (OR = 8.81; 95% CI = 2.58 to 30.05), known clinical vascular disease (OR = 7.50; 95% CI = 2.88 to 19.55), home visit requested (OR = 7.31; 95% CI = 2.27 to 23.57), and known heart failure (OR = 3.53; 95% CI = 1.14 to 10.96).
Conclusion: Although individual criteria were only moderately effective, in combination they can help to decide about further management of patients with chest pain in primary care.
Figures
References
-
- Ruigomez A, Rodriguez LA, Wallander MA, et al. Chest pain in general practice: incidence, comorbidity and mortality. Fam Pract. 2006;23(2):167–174. - PubMed
-
- Buntinx F, Knockaert D, Bruyninckx R, et al. Chest pain in general practice or in the hospital emergency department: is it the same? Fam Pract. 2001;18(6):586–589. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials