

Laparoscopic-assisted percutaneous endoscopic gastrostomy tube placement
- PMID: 20529530
- PMCID: PMC3021284
- DOI: 10.4293/108680810X12674612014662
Laparoscopic-assisted percutaneous endoscopic gastrostomy tube placement
Abstract
Background: Percutaneous endoscopic gastrostomy (PEG) is the most common way of placing a feeding tube. Sometimes PEG cannot be used to safely place a feeding tube, most commonly secondary to an inability to transilluminate the abdominal wall. Whereas open gastrostomy was previously necessary in such cases, laparoscopic-assisted percutaneous endoscopic gastrostomy (LAPEG) is a viable option and is reviewed here.
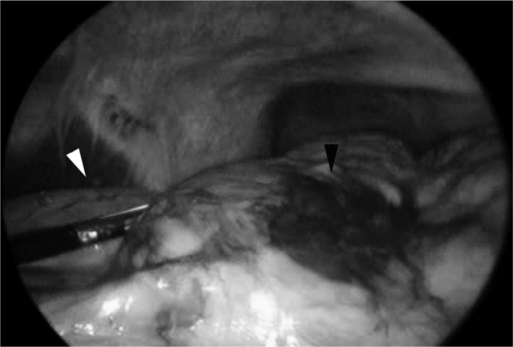
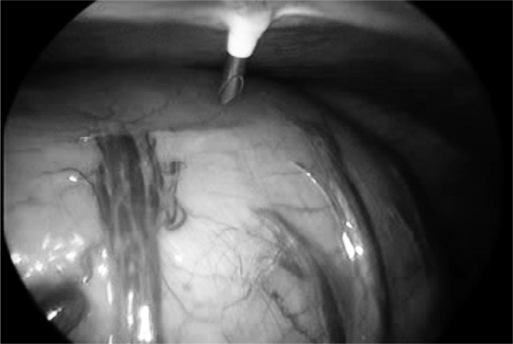
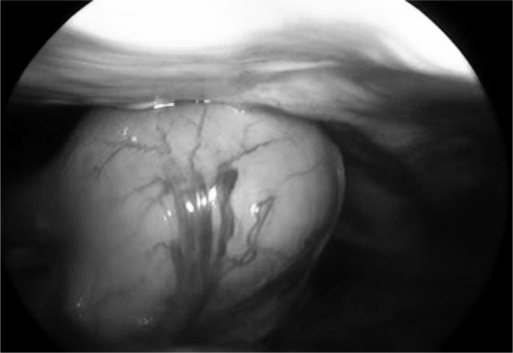
Methods: All patients referred for surgical feeding tube placement after unsuccessful PEG were considered for LAPEG. A diagnostic laparoscopy was performed to identify the reason for the failed PEG attempt. Additional ports were placed as needed for the retraction of organs and lysis of adhesions. The stomach was visualized, and the PEG was placed.
Results: Eight patients who underwent an unsuccessful PEG were taken to the operating room for LAPEG. All patients had successful LAPEG placement. No postoperative complications occurred. The most common reason identified for failed PEG attempt was adhesions followed by overlying organs. Average OR time was 32 minutes.
Conclusion: When conventional PEG placement is not possible, LAPEG placement should be considered as a time efficient, minimally invasive alternative to open gastrostomy.
Figures
Similar articles
-
Laparoscopic-assisted percutaneous endoscopic gastrostomy in two patients who failed percutaneous endoscopic gastrostomy.Int J Surg Case Rep. 2015;13:40-2. doi: 10.1016/j.ijscr.2015.06.002. Epub 2015 Jun 6. Int J Surg Case Rep. 2015. PMID: 26101053 Free PMC article.
-
Clinical Evaluation of Laparoscopic-Assisted Percutaneous Endoscopic Gastrostomy (LAPEG).Int Surg. 2015 Jun;100(6):1144-7. doi: 10.9738/INTSURG-D-14-00261.1. Epub 2015 Jan 6. Int Surg. 2015. PMID: 25563858 Free PMC article.
-
Laparoendoscopic Percutaneous Endoscopic Gastrostomy in Adults.J Laparoendosc Adv Surg Tech A. 2018 Oct;28(10):1192-1195. doi: 10.1089/lap.2018.0119. Epub 2018 Jun 20. J Laparoendosc Adv Surg Tech A. 2018. PMID: 29924677
-
Laparoscopic-Assisted Percutaneous Endoscopic Gastrostomy.Curr Gastroenterol Rep. 2016 Sep;18(9):46. doi: 10.1007/s11894-016-0520-2. Curr Gastroenterol Rep. 2016. PMID: 27422123 Review.
-
Laparoscopic gastrostomy and jejunostomy.J Long Term Eff Med Implants. 2004;14(1):1-11. doi: 10.1615/jlongtermeffmedimplants.v14.i1.10. J Long Term Eff Med Implants. 2004. PMID: 14961758 Review.
Cited by
-
Laparoscopically assisted percutaneous endoscopic gastrostomy performed for remnant stomach in patient with amyotrophic lateral sclerosis: a case report.Surg Case Rep. 2023 Jun 7;9(1):98. doi: 10.1186/s40792-023-01683-y. Surg Case Rep. 2023. PMID: 37280445 Free PMC article.
-
Laparoscopic-assisted percutaneous endoscopic gastrostomy in two patients who failed percutaneous endoscopic gastrostomy.Int J Surg Case Rep. 2015;13:40-2. doi: 10.1016/j.ijscr.2015.06.002. Epub 2015 Jun 6. Int J Surg Case Rep. 2015. PMID: 26101053 Free PMC article.
-
Relationship of early acute complications and insertion site in push method percutaneous endoscopic gastrostomy.Sci Rep. 2020 Nov 25;10(1):20551. doi: 10.1038/s41598-020-77553-6. Sci Rep. 2020. PMID: 33239745 Free PMC article.
-
Laparoscopic Percutaneous Endoscopic Gastrostomy Is Useful for Elderly.JSLS. 2019 Apr-Jun;23(2):e2019.00011. doi: 10.4293/JSLS.2019.00011. JSLS. 2019. PMID: 31148916 Free PMC article.
-
Gastrostomy tubes: Fundamentals, periprocedural considerations, and best practices.World J Gastrointest Surg. 2022 Apr 27;14(4):286-303. doi: 10.4240/wjgs.v14.i4.286. World J Gastrointest Surg. 2022. PMID: 35664365 Free PMC article. Review.
References
-
- Gauderer M, Ponsky J, Izant R. Gastrostomy without laparotomy: a percutaneous endoscopic technique. J Pediatr Surg. 1980;15:872–875 - PubMed
-
- Gauderer M. Percutaneous endoscopic gastrostomy-20 years later: a historical perspective. J Pediatr Surg. 2001;36(1):217–219 - PubMed
-
- Prosser B. Common issues in PEG tubes-what every fellow should know. Gastrointest Endosc. 2006;64(6):970–972 - PubMed
-
- Denzer U, Mergener K, Kanzler S, et al. Mini-laparoscopically guided percutaneous gastrostomy and jejunostomy. Gastrointest Endosc. 2003;58(3):434–438 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources