

Intrinsic cardiac nerve activity and paroxysmal atrial tachyarrhythmia in ambulatory dogs
- PMID: 20529998
- PMCID: PMC2890034
- DOI: 10.1161/CIRCULATIONAHA.109.919829
Intrinsic cardiac nerve activity and paroxysmal atrial tachyarrhythmia in ambulatory dogs
Abstract
Background: Little is known about the relationship between intrinsic cardiac nerve activity (ICNA) and spontaneous arrhythmias in ambulatory animals.
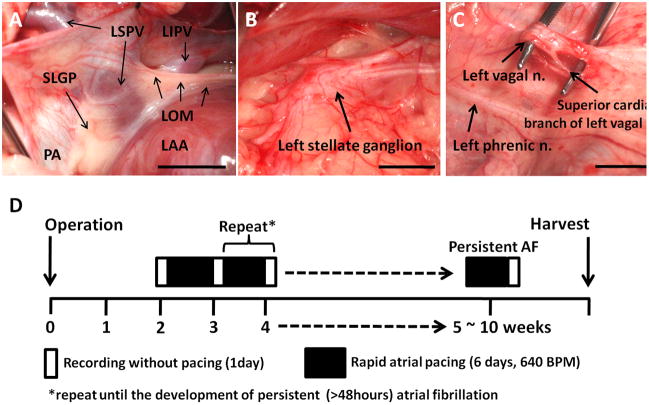
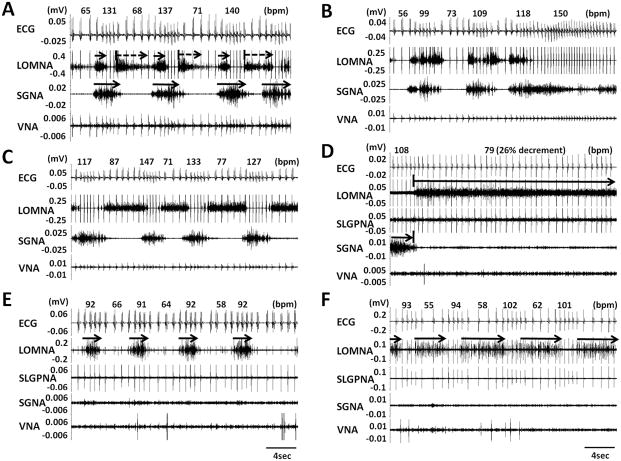
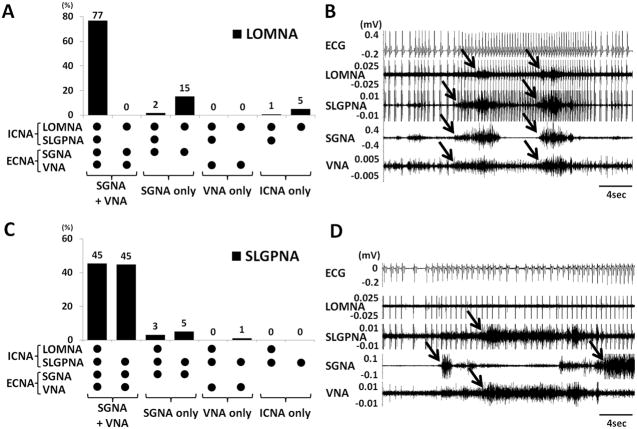
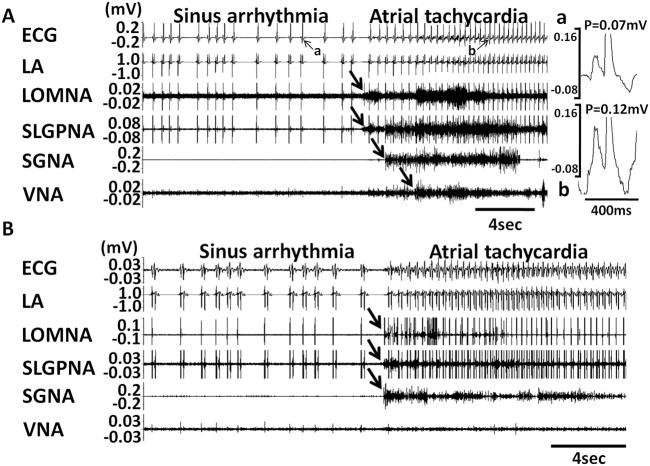
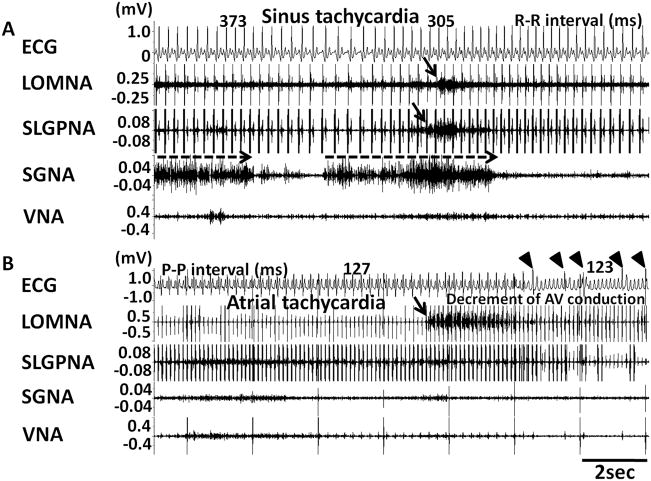
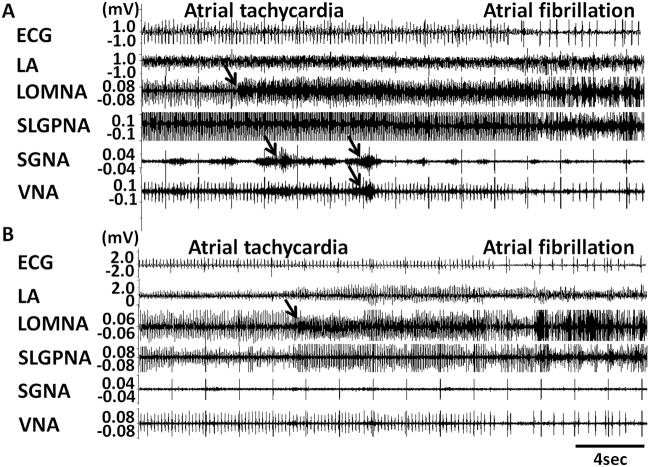
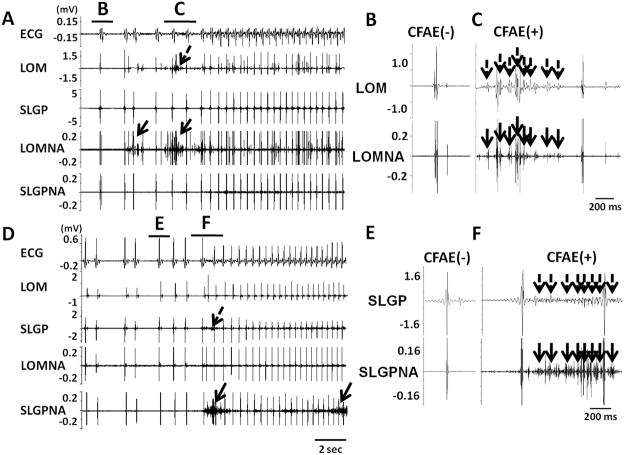
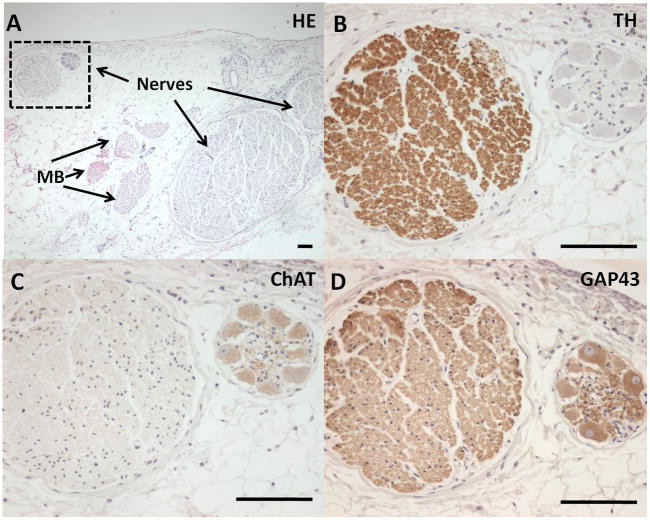
Methods and results: We implanted radiotransmitters to record extrinsic cardiac nerve activity (ECNA; including stellate ganglion nerve activity and vagal nerve activity) and ICNA (including superior left ganglionated plexi nerve activity and ligament of Marshall nerve activity) in 6 ambulatory dogs. Intermittent rapid left atrial pacing was performed to induce paroxysmal atrial fibrillation or atrial tachycardia. The vast majority (94%) of ligament of Marshall nerve activity were preceded by or coactivated with ECNA (stellate ganglion nerve activity or vagal nerve activity), whereas 6% of episodes were activated alone without concomitant stellate ganglion nerve activity or vagal nerve activity. Paroxysmal atrial fibrillation and atrial tachycardia were invariably (100%) preceded (<5 seconds) by ICNA. Most paroxysmal atrial tachycardia events (89%) were preceded by ICNA and sympathovagal coactivation, whereas 11% were preceded by ICNA and stellate ganglion nerve activity-only activation. Most paroxysmal atrial fibrillation events were preceded only by ICNA (72%); the remaining 28% were preceded by ECNA and ICNA together. Complex fractionated atrial electrograms were observed during ICNA discharges that preceded the onset of paroxysmal atrial tachycardia and atrial fibrillation. Immunostaining confirmed the presence of both adrenergic and cholinergic nerve at ICNA sites.
Conclusions: There is a significant temporal relationship between ECNA and ICNA. However, ICNA can also activate alone. All paroxysmal atrial tachycardia and atrial fibrillation episodes were invariably preceded by ICNA. These findings suggest that ICNA (either alone or in collaboration with ECNA) is an invariable trigger of paroxysmal atrial tachyarrhythmias. ICNA might contaminate local atrial electrograms, resulting in complex fractionated atrial electrogram-like activity.
Conflict of interest statement
Dr Xiaohong Zhou of Medtronic Inc. donated equipment used in these studies.
Figures
Similar articles
-
Neural mechanisms of paroxysmal atrial fibrillation and paroxysmal atrial tachycardia in ambulatory canines.Circulation. 2008 Aug 26;118(9):916-25. doi: 10.1161/CIRCULATIONAHA.108.776203. Epub 2008 Aug 12. Circulation. 2008. PMID: 18697820 Free PMC article.
-
Left stellate ganglion and vagal nerve activity and cardiac arrhythmias in ambulatory dogs with pacing-induced congestive heart failure.J Am Coll Cardiol. 2007 Jul 24;50(4):335-43. doi: 10.1016/j.jacc.2007.03.045. Epub 2007 Jul 10. J Am Coll Cardiol. 2007. PMID: 17659201
-
Cryoablation of stellate ganglia and atrial arrhythmia in ambulatory dogs with pacing-induced heart failure.Heart Rhythm. 2009 Dec;6(12):1772-9. doi: 10.1016/j.hrthm.2009.08.011. Epub 2009 Aug 13. Heart Rhythm. 2009. PMID: 19959128 Free PMC article.
-
Ganglionated plexi as neuromodulation targets for atrial fibrillation.J Cardiovasc Electrophysiol. 2017 Dec;28(12):1485-1491. doi: 10.1111/jce.13319. Epub 2017 Sep 8. J Cardiovasc Electrophysiol. 2017. PMID: 28833764 Free PMC article. Review.
-
Autonomic nerve activity and atrial fibrillation.Heart Rhythm. 2007 Mar;4(3 Suppl):S61-4. doi: 10.1016/j.hrthm.2006.12.006. Epub 2006 Dec 15. Heart Rhythm. 2007. PMID: 17336887 Free PMC article. Review.
Cited by
-
Atrial Myopathy.JACC Basic Transl Sci. 2019 Sep 23;4(5):640-654. doi: 10.1016/j.jacbts.2019.05.005. eCollection 2019 Sep. JACC Basic Transl Sci. 2019. PMID: 31768479 Free PMC article. Review.
-
Effect of the stellate ganglion on atrial fibrillation and atrial electrophysiological properties and its left-right asymmetry in a canine model.Exp Clin Cardiol. 2013 Winter;18(1):38-42. Exp Clin Cardiol. 2013. PMID: 24294036 Free PMC article.
-
Simultaneous recordings of intrinsic cardiac nerve activity and skin sympathetic nerve activity from human patients during the postoperative period.Heart Rhythm. 2017 Nov;14(11):1587-1593. doi: 10.1016/j.hrthm.2017.06.030. Epub 2017 Jun 23. Heart Rhythm. 2017. PMID: 28648667 Free PMC article.
-
Predictive factors and prevalence of microalbuminuria in HIV-infected patients: a cross-sectional analysis.BMC Nephrol. 2017 Jul 28;18(1):255. doi: 10.1186/s12882-017-0672-9. BMC Nephrol. 2017. PMID: 28754089 Free PMC article.
-
Patterns of baseline autonomic nerve activity and the development of pacing-induced sustained atrial fibrillation.Heart Rhythm. 2011 Apr;8(4):583-9. doi: 10.1016/j.hrthm.2010.11.040. Epub 2010 Nov 29. Heart Rhythm. 2011. PMID: 21118728 Free PMC article.
References
-
- Marshall J. On the development of the great anterior veins in man and mammalia: including an account of certain remnants of foetal structure found in the adult, a comparative view of these great veins in the different mammalia, and an analysis of their occasional peculiarities in the human subject. Phil Trans R Soc Lond. 1850;140:133–169.
-
- Scherlag BJ, Yeh BK, Robinson MJ. Inferior interatrial pathway in the dog. Circulation Research. 1972;31:18–35. - PubMed
-
- Doshi RN, Wu TJ, Yashima M, Kim YH, Ong JJC, Cao JM, Hwang C, Yashar P, Fishbein MC, Karagueuzian HS, Chen PS. Relation between ligament of Marshall and adrenergic atrial tachyarrhythmia. Circulation. 1999;100:876–883. - PubMed
-
- Armour JA, Richer LP, Page P, Vinet A, Kus T, Vermeulen M, Nadeau R, Cardinal R. Origin and pharmacological response of atrial tachyarrhythmias induced by activation of mediastinal nerves in canines. Auton Neurosci. 2005;118:68–78. - PubMed
-
- Ulphani JS, Arora R, Cain JH, Villuendas R, Shen S, Gordon D, Inderyas F, Harvey LA, Morris A, Goldberger JJ, Kadish AH. The ligament of Marshall as a parasympathetic conduit. Am J Physiol Heart Circ Physiol. 2007;293:H1629–H1635. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
