

Respiratory morbidity and lung function in preterm infants of 32 to 36 weeks' gestational age
- PMID: 20530073
- PMCID: PMC3000351
- DOI: 10.1542/peds.2009-1381
Respiratory morbidity and lung function in preterm infants of 32 to 36 weeks' gestational age
Abstract
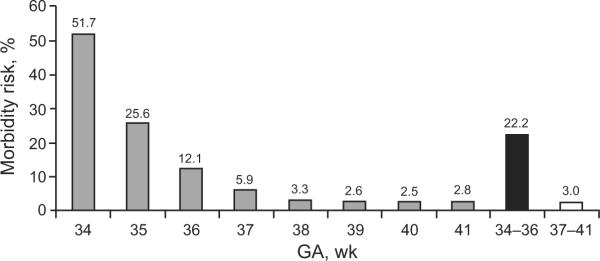
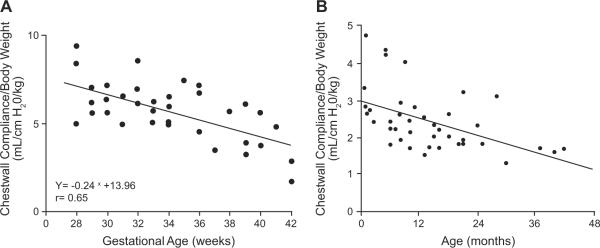
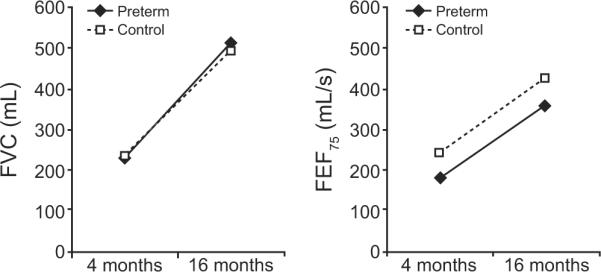
Normal lung development follows a series of orchestrated events. Premature birth interrupts normal in utero lung development, which results in significant alterations in lung function and physiology. Increasingly, there are reports documenting the broad range of complications experienced by infants aged 34 to 36 weeks' gestational age (GA). Our objective was to summarize the evidence demonstrating respiratory system vulnerability in infants aged 34 to 36 weeks' GA and to review the developmental and physiologic principles that underlie this vulnerability. A comprehensive search for studies that reported epidemiologic data and respiratory morbidity was conducted on the PubMed, Medline, Ovid Biosis, and Embase databases from 2000 to 2009 by using medical subject headings "morbidity in late preterm infants," "preterm infants and lung development," "prematurity and morbidity," and "prematurity and lung development." Because the number of studies exclusive to infants aged 34 to 36 weeks' GA was limited, selected studies also included infants aged 32 to 36 weeks' GA. Of the 24 studies identified, 16 were retrospective population-based cohort studies; 8 studies were observational. These studies consistently revealed that infants born at 32 to 36 weeks' GA, including infants of 34 to 36 weeks' GA, experience substantial respiratory morbidity compared with term infants. Levels of morbidity were, at times, comparable to those observed in very preterm infants. The developmental and physiologic mechanisms that underlie the increased morbidity rate and alterations in respiratory function are discussed. We also present evidence to demonstrate that the immaturity of the respiratory system of infants 34 to 36 weeks' GA at birth results in increased morbidity in infancy and leads to deficits in lung function that may persist into adulthood.
Figures
References
-
- Hamilton BE, Martin JA, Ventura SJ. Births: preliminary data for 2007. Natl Vital Stat Rep. 2009;57(12):1–23. - PubMed
-
- American College of Obstetricians and Gynecologists ACOG educational bulletin. Assessment of fetal lung maturity. Number 230, November 1996. Committee on Educational Bulletins of the American College of Obstetricians and Gynecologists. Int J Gynaecol Obstet. 1997;56(2):191–198. - PubMed
-
- American College of Obstetricians and Gynecologists ACOG committee opinion: antenatal corticosteroid therapy for fetal maturation. Obstet Gynecol. 2002;99(5 pt 1):871–873. - PubMed
-
- Kramer MS, Demissie K, Yang H, Platt RW, Sauvé R, Liston R. The contribution of mild and moderate preterm birth to infant mortality. Fetal and Infant Health Study Group of the Canadian Perinatal Surveillance System. JAMA. 2000;284(7):843–849. - PubMed
-
- Santos IS, Matijasevich A, Silveira MF, et al. Associated factors and consequences of late preterm births: results from the 2004 Pelotas birth cohort. Paediatr Perinat Epidemiol. 2008;22(4):350–359. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
