

Human papillomavirus and survival of patients with oropharyngeal cancer
- PMID: 20530316
- PMCID: PMC2943767
- DOI: 10.1056/NEJMoa0912217
Human papillomavirus and survival of patients with oropharyngeal cancer
Abstract
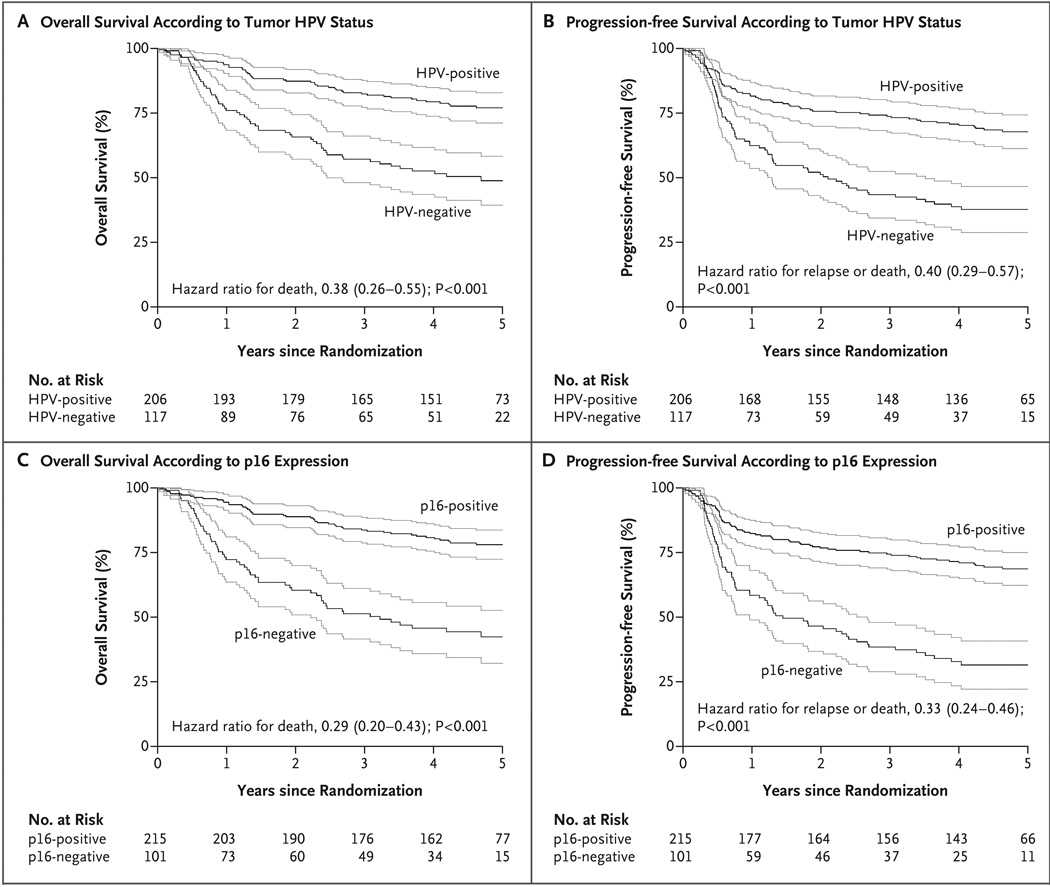
Background: Oropharyngeal squamous-cell carcinomas caused by human papillomavirus (HPV) are associated with favorable survival, but the independent prognostic significance of tumor HPV status remains unknown.
Methods: We performed a retrospective analysis of the association between tumor HPV status and survival among patients with stage III or IV oropharyngeal squamous-cell carcinoma who were enrolled in a randomized trial comparing accelerated-fractionation radiotherapy (with acceleration by means of concomitant boost radiotherapy) with standard-fractionation radiotherapy, each combined with cisplatin therapy, in patients with squamous-cell carcinoma of the head and neck. Proportional-hazards models were used to compare the risk of death among patients with HPV-positive cancer and those with HPV-negative cancer.
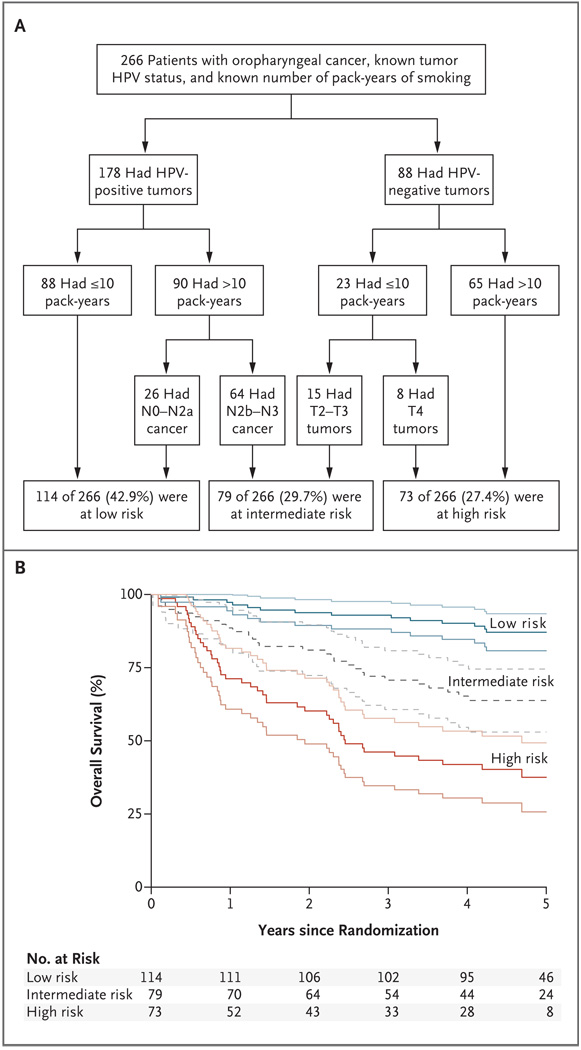
Results: The median follow-up period was 4.8 years. The 3-year rate of overall survival was similar in the group receiving accelerated-fractionation radiotherapy and the group receiving standard-fractionation radiotherapy (70.3% vs. 64.3%; P=0.18; hazard ratio for death with accelerated-fractionation radiotherapy, 0.90; 95% confidence interval [CI], 0.72 to 1.13), as were the rates of high-grade acute and late toxic events. A total of 63.8% of patients with oropharyngeal cancer (206 of 323) had HPV-positive tumors; these patients had better 3-year rates of overall survival (82.4%, vs. 57.1% among patients with HPV-negative tumors; P<0.001 by the log-rank test) and, after adjustment for age, race, tumor and nodal stage, tobacco exposure, and treatment assignment, had a 58% reduction in the risk of death (hazard ratio, 0.42; 95% CI, 0.27 to 0.66). The risk of death significantly increased with each additional pack-year of tobacco smoking. Using recursive-partitioning analysis, we classified our patients as having a low, intermediate, or high risk of death on the basis of four factors: HPV status, pack-years of tobacco smoking, tumor stage, and nodal stage.
Conclusions: Tumor HPV status is a strong and independent prognostic factor for survival among patients with oropharyngeal cancer. (ClinicalTrials.gov number, NCT00047008.)
2010 Massachusetts Medical Society
Figures
Comment in
-
Prognostic implications of HPV in oropharyngeal cancer.N Engl J Med. 2010 Jul 1;363(1):82-4. doi: 10.1056/NEJMe1003607. Epub 2010 Jun 7. N Engl J Med. 2010. PMID: 20530315 No abstract available.
-
Human papillomavirus—a powerful predictor of survival in patients with oropharyngeal cancer.Nat Rev Clin Oncol. 2010 Sep;7(9):481. doi: 10.1038/nrclinonc.2010.124. Nat Rev Clin Oncol. 2010. PMID: 20824898 No abstract available.
-
Human papillomavirus and oropharyngeal cancer survival.N Engl J Med. 2010 Oct 14;363(16):1576. doi: 10.1056/NEJMc1008419. N Engl J Med. 2010. PMID: 20942677 No abstract available.
-
Human papillomavirus and oropharyngeal cancer survival.N Engl J Med. 2010 Oct 14;363(16):1576. doi: 10.1056/NEJMc1008419. N Engl J Med. 2010. PMID: 20949668 No abstract available.
-
Do conventional treatments for HPV-positive head and neck cancers elicit immunotherapeutic type responses?Immunotherapy. 2011 Apr;3(4):469-73. doi: 10.2217/imt.11.25. Immunotherapy. 2011. PMID: 21463187 No abstract available.
-
Human papillomavirus and oropharyngeal cancer: shifting paradigms and exploring opportunities.Natl Med J India. 2011 Mar-Apr;24(2):88-90. Natl Med J India. 2011. PMID: 21668052 No abstract available.
References
-
- Gillison M, D’Souza G, Westra W, et al. Distinct risk factor profiles for human papillomavirus type 16-positive and human papillomavirus 16-negative head and neck cancers. J Natl Cancer Inst. 2008;100:407–420. - PubMed
-
- Rampias T, Sasaki C, Weinberger P, Psyrri A. E6 and E7 gene silencing and transformed phenotype of human papillomavirus 16-positive oropharyngeal cancer cells. J Natl Cancer Inst. 2009;101:412–423. - PubMed
-
- Ragin CC, Taioli E. Survival of squamous cell carcinoma of the head and neck in relation to human papillomavirus infection: review and meta-analysis. Int J Cancer. 2007;121:1813–1820. - PubMed
-
- Fakhry C, Westra WH, Li S, et al. Improved survival of patients with human papillomavirus-positive head and neck squamous cell carcinoma in a prospective clinical trial. J Natl Cancer Inst. 2008;100:261–269. - PubMed
-
- Bourhis J, Overgaard J, Audry H, et al. Hyperfractionated or accelerated radiotherapy in head and neck cancer: a meta-analysis. Lancet. 2006;368:843–854. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical