

Colorectal cancer incidence trends in the United States and United kingdom: evidence of right- to left-sided biological gradients with implications for screening
- PMID: 20530677
- PMCID: PMC2914859
- DOI: 10.1158/0008-5472.CAN-09-4417
Colorectal cancer incidence trends in the United States and United kingdom: evidence of right- to left-sided biological gradients with implications for screening
Abstract
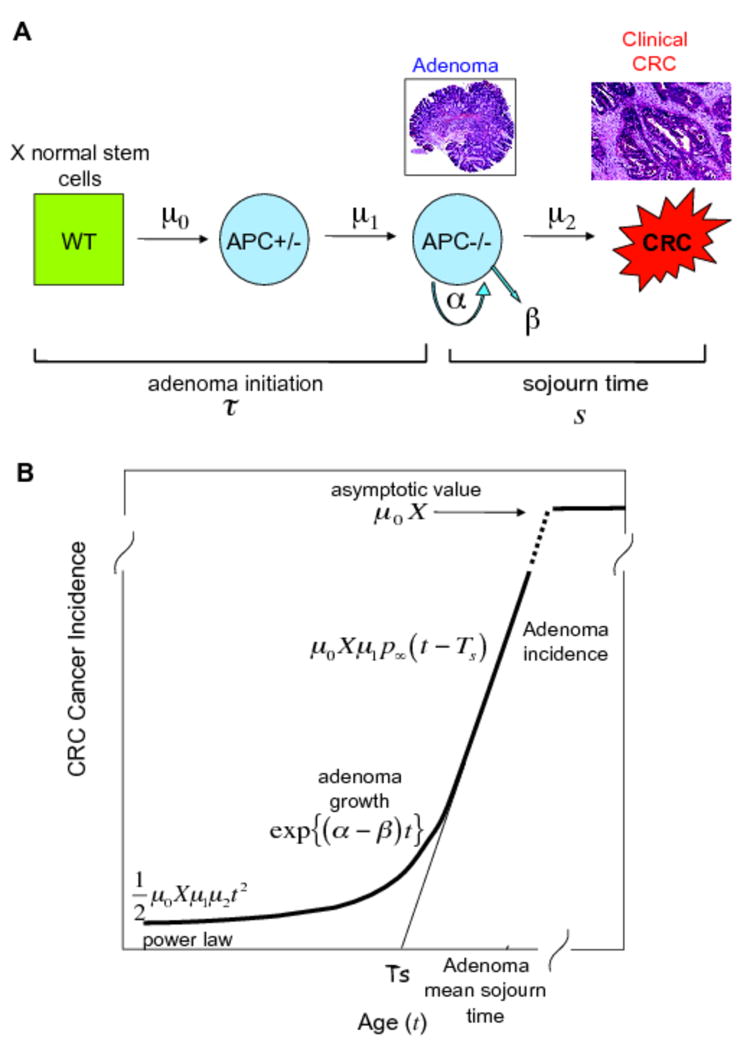
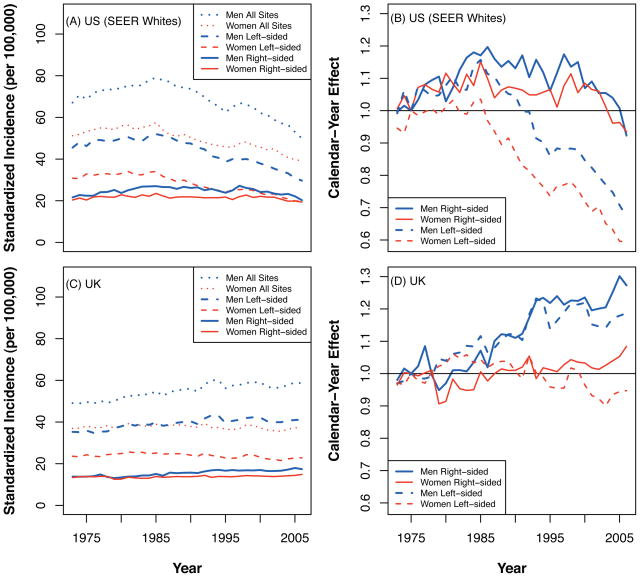
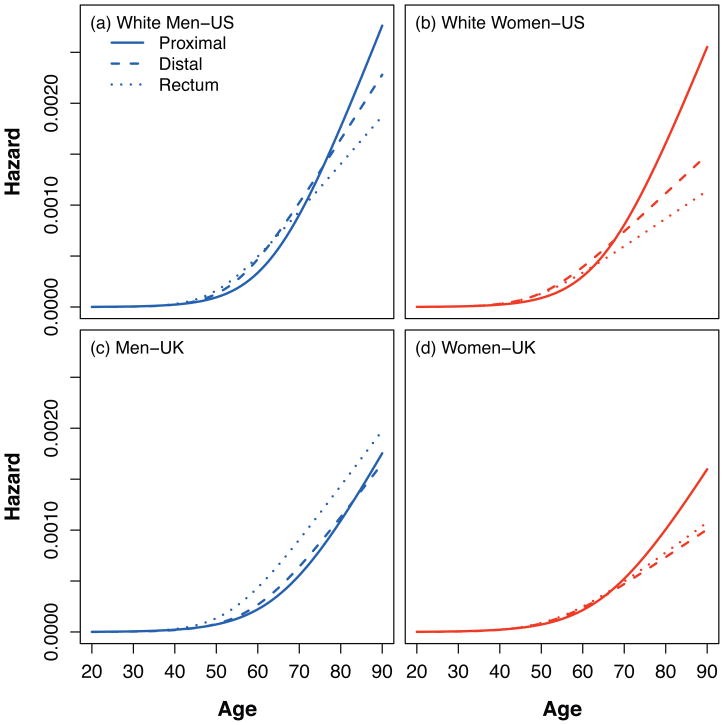
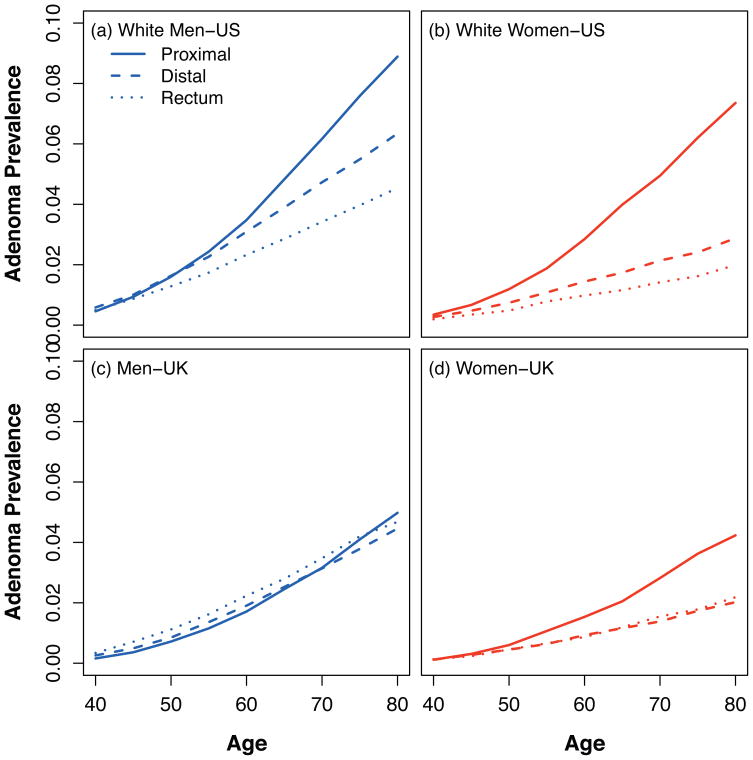
Several lines of evidence support the premise that screening colonoscopy reduces colorectal cancer (CRC) incidence, but there may be differential benefits for right- and left-sided tumors. To better understand the biological basis of this differential effect, we derived biomathematical models of CRC incidence trends in U.S. and U.K. populations, representing relatively high- and low-prevalence screening, respectively. Using the Surveillance Epidemiology and End Results (SEER) and the Office for National Statistics (ONS) registries (both 1973-2006), we derived stochastic multistage clonal expansion (MSCE) models for right-sided (proximal colon) and left-sided (distal colon and rectal) tumors. The MSCE concept is based on the initiation-promotion-progression paradigm of carcinogenesis and provides a quantitative description of natural tumor development from the initiation of an adenoma (via biallelic tumor suppressor gene inactivation) to the clinical detection of CRC. From 1,228,036 (SEER: 340,582; ONS: 887,454) cases, parameter estimates for models adjusted for calendar-year and birth-cohort effects showed that adenoma initiation rates were higher for right-sided tumors, whereas, paradoxically, adenoma growth rates were higher for left-sided tumors. The net effect was a higher cancer risk in the right colon only after age 70 years. Consistent with this finding, simulations of adenoma development predicted that the relative prevalence for right- versus left-sided tumors increases with increasing age, a differential effect most striking in women. Using a realistic biomathematical description of CRC development for two nationally representative registries, we show age- and sex-dependent biological gradients for right- and left-sided colorectal tumors. These findings argue for an age-, sex-, and site-directed approach to CRC screening.
Copyright 2010 AACR.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- American Cancer Society. Colorectal Cancer Facts & Figures. 2008–2010. [accessed 4th March 2010]. http://www.cancer.org/downloads/STT/F861708_finalforweb.pdf.
-
- Cancer Research UK Cancer Statistics. [accessed 4th March 2010]. http://info.cancerresearchuk.org/cancerstats/incidence/index.htm.
-
- Mandel JS, Bond JH, Church TR, et al. Reducing mortality from colorectal cancer by screening for fecal occult blood. minnesota colon cancer control study. N Engl J Med. 1993;328(19):1365–71. - PubMed
-
- Modeling to guide public health research and priorities. Cancer Intervention and Surveillance Modeling Network. [accessed 4th March 2010]. http://cisnet.cancer.gov/colorectal/
-
- Muller AD, Sonnenberg A. Protection by endoscopy against death from colorectal cancer. A case-control study among veterans. Arch Intern Med. 1995;155(16):1741–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
