

Biobehavioral, immune, and health benefits following recurrence for psychological intervention participants
- PMID: 20530702
- PMCID: PMC2910547
- DOI: 10.1158/1078-0432.CCR-10-0278
Biobehavioral, immune, and health benefits following recurrence for psychological intervention participants
Erratum in
- Clin Cancer Res. 2010 Sep 1;16(17):4490
Abstract
Purpose: A clinical trial was designed to test the hypothesis that a psychological intervention could reduce the risk of cancer recurrence. Newly diagnosed regional breast cancer patients (n = 227) were randomized to the intervention-with-assessment or the assessment-only arm. The intervention had positive psychological, social, immune, and health benefits, and after a median of 11 years the intervention arm was found to have reduced the risk of recurrence (hazard ratio, 0.55; P = 0.034). In follow-up, we hypothesized that the intervention arm might also show longer survival after recurrence. If observed, we then would examine potential biobehavioral mechanisms.
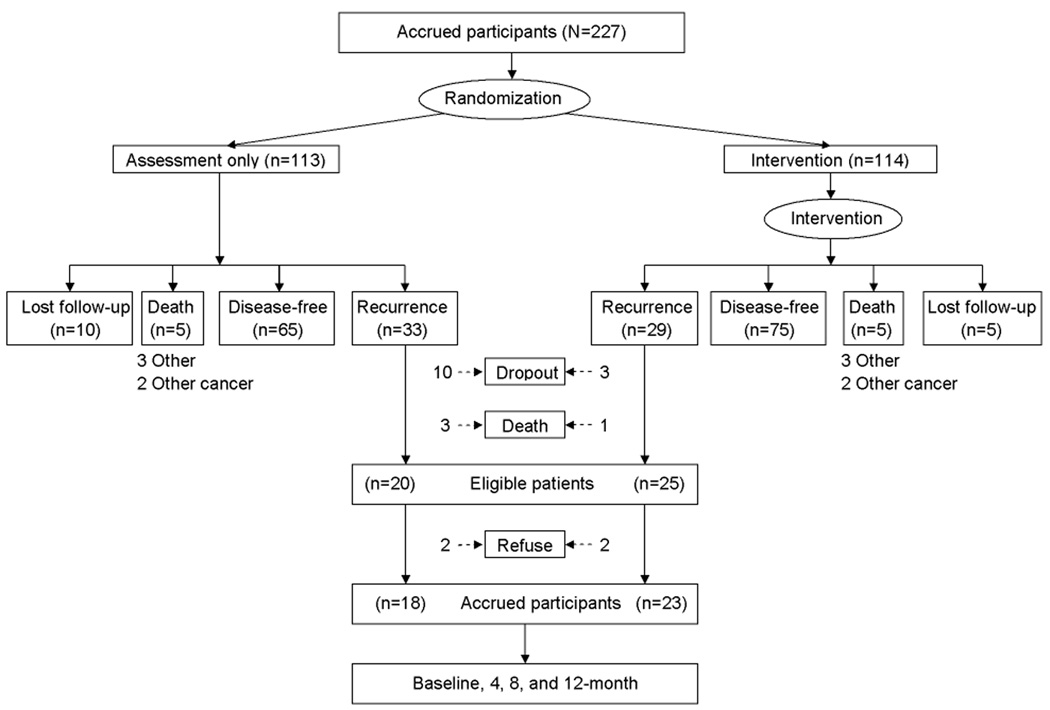
Experimental design: All patients were followed; 62 recurred. Survival analyses included all 62. Upon recurrence diagnosis, those available for further biobehavioral study were accrued (n = 41, 23 intervention and 18 assessment). For those 41, psychological, social, adherence, health, and immune (natural killer cell cytotoxicity, T-cell proliferation) data were collected at recurrence diagnosis and 4, 8, and 12 months later.
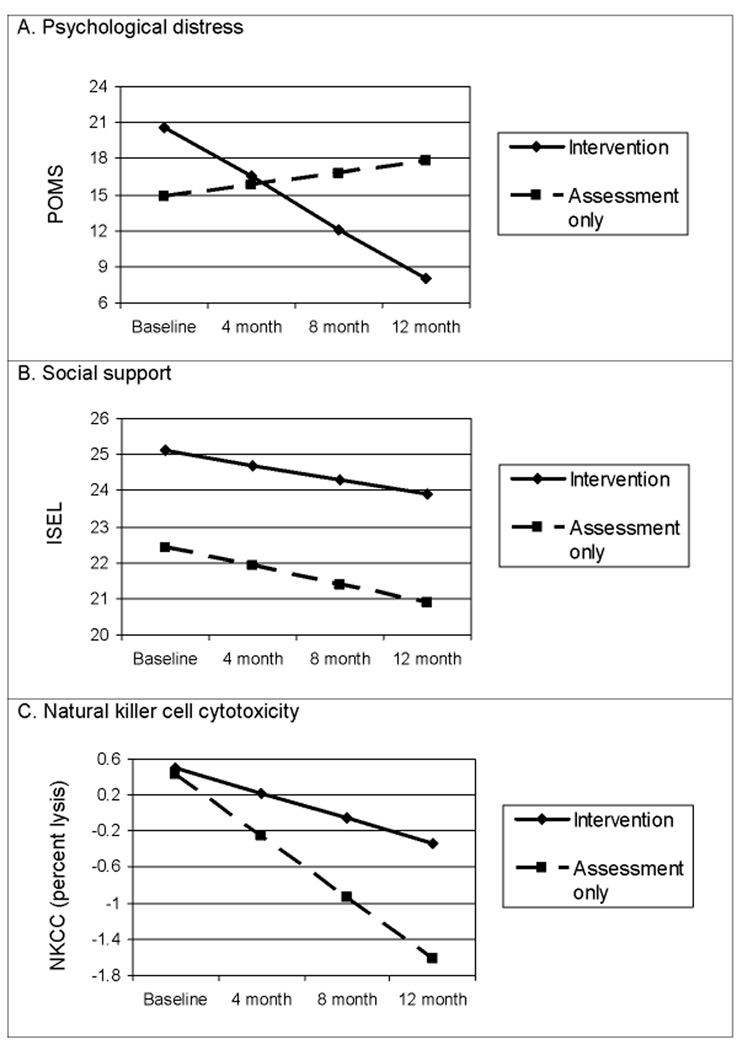
Results: Intent-to-treat analysis revealed reduced risk of death following recurrence for the intervention arm (hazard ratio, 0.41; P = 0.014). Mixed-effects follow-up analyses with biobehavioral data showed that all patients responded with significant psychological distress at recurrence diagnosis, but thereafter only the intervention arm improved (P values < 0.023). Immune indices were significantly higher for the intervention arm at 12 months (P values < 0.017).
Conclusions: Hazards analyses augment previous findings in showing improved survival for the intervention arm after recurrence. Follow-up analyses showing biobehavioral advantages for the intervention arm contribute to our understanding of how improved survival was achieved.
(c) 2010 AACR.
Conflict of interest statement
Figures

Comment in
-
Psychologic intervention and survival: wishing does not make it so--letter.Clin Cancer Res. 2010 Nov 1;16(21):5364-5. doi: 10.1158/1078-0432.CCR-10-1703. Epub 2010 Oct 19. Clin Cancer Res. 2010. PMID: 20959406 No abstract available.
References
-
- Chida Y, Hamer M, Wardle J, Steptoe A. Do stress-related psychological factors contribute to cancer incidence and survival: A systematic review and meta-analysis. Nat Clin Pract Oncol. 2008;5(8):466–475. - PubMed
-
- Quinten C, Coens C, Mauer M, et al. Baseline quality of life as a prognostic indicator of survival: a meta-analysis of individual patient data from EORTC clinical trials. Lancet Oncol. 2009;10(9):865–871. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
