

Fenofibric acid: a new fibrate approved for use in combination with statin for the treatment of mixed dyslipidemia
- PMID: 20531954
- PMCID: PMC2879297
- DOI: 10.2147/vhrm.s6714
Fenofibric acid: a new fibrate approved for use in combination with statin for the treatment of mixed dyslipidemia
Abstract
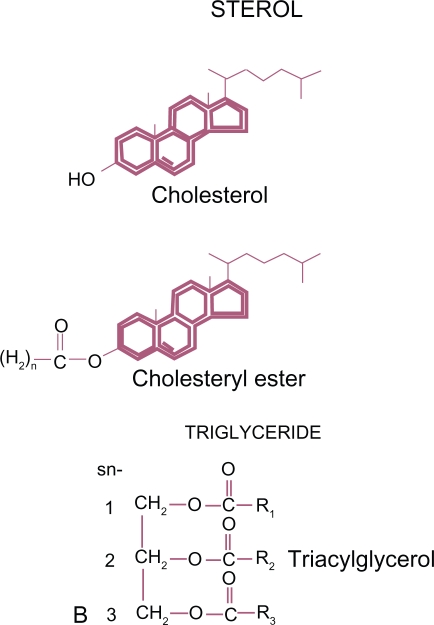
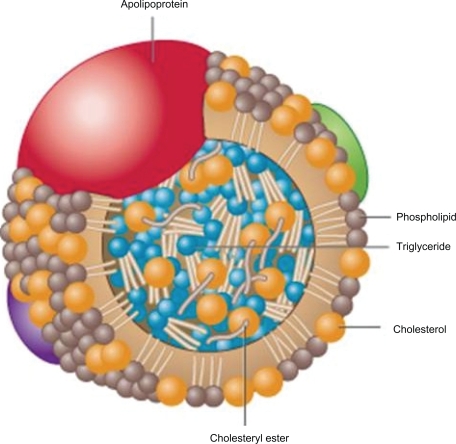
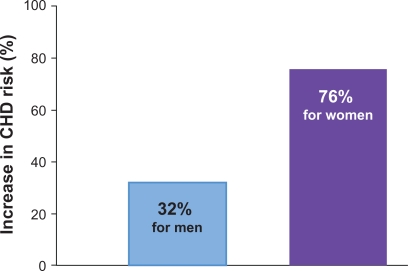
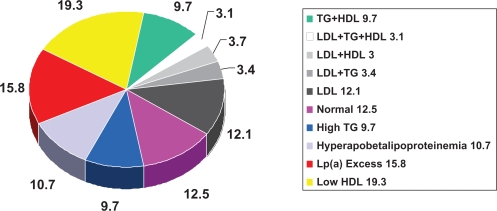
The last two to three decades have seen an explosive growth in interest and information regarding cardiovascular disease (CVD) risk assessment and treatment. Evidence for the role of low-density lipoprotein (LDL) in risk has led to a series of clinical guidelines/recommendations on the importance of LDL lowering with statin treatment. There is also substantial evidence on a number of lipoproteins in the initiation and progression of atherosclerosis and CV events. Health care professionals have not embraced easily novel approaches to identifying those at increased risk and more aggressive treatment. This is especially true for non-LDL factors. The use of non-statin drugs such as fibrates has been modest and many health care professionals avoid consideration of combination therapy due to an inordinate fear of toxicity. This review will attempt to provide appropriate background information on lipids/lipoproteins, including non-high density lipoprotein and risk, as well as data available on fibrates and combination pharmacologic therapy. We will review a new agent, TriLipix((R)) (fenofibric acid), and its potential role in treatment.
Keywords: TriLipix; dyslipidemia; fenofibric acid; fibrate; non-high density lipoprotein; peroxisome proliferated activated receptors; triglycerides; very-low-density lipoprotein.
Figures
Similar articles
-
Management of dyslipidemias with fibrates, alone and in combination with statins: role of delayed-release fenofibric acid.Vasc Health Risk Manag. 2010 Aug 9;6:525-39. doi: 10.2147/vhrm.s5593. Vasc Health Risk Manag. 2010. PMID: 20730069 Free PMC article. Review.
-
Efficacy and safety of fenofibric acid co-administered with low- or moderate-dose statin in patients with mixed dyslipidemia and type 2 diabetes mellitus: results of a pooled subgroup analysis from three randomized, controlled, double-blind trials.Am J Cardiovasc Drugs. 2010;10(2):73-84. doi: 10.2165/10061630-000000000-00000. Am J Cardiovasc Drugs. 2010. PMID: 20136164
-
Fibrates are an essential part of modern anti-dyslipidemic arsenal: spotlight on atherogenic dyslipidemia and residual risk reduction.Cardiovasc Diabetol. 2012 Oct 11;11:125. doi: 10.1186/1475-2840-11-125. Cardiovasc Diabetol. 2012. PMID: 23057687 Free PMC article. Review.
-
"If it ain't broke, don't fix it": a commentary on the positive-negative results of the ACCORD Lipid study.Cardiovasc Diabetol. 2010 Jun 15;9:24. doi: 10.1186/1475-2840-9-24. Cardiovasc Diabetol. 2010. PMID: 20550659 Free PMC article.
-
The role of a new formulation of fenofibric acid in the treatment of mixed dyslipidemia in type 2 diabetes.Drugs Today (Barc). 2010 Oct;46(10):757-64. doi: 10.1358/dot.2010.46.10.1519652. Drugs Today (Barc). 2010. PMID: 21076712 Review.
Cited by
-
A Mendelian randomization study for drug repurposing reveals bezafibrate and fenofibric acid as potential osteoporosis treatments.Front Pharmacol. 2023 Jul 20;14:1211302. doi: 10.3389/fphar.2023.1211302. eCollection 2023. Front Pharmacol. 2023. PMID: 37547327 Free PMC article.
-
Fibrates as therapy for osteoarthritis and rheumatoid arthritis? A systematic review.Ther Adv Musculoskelet Dis. 2013 Feb;5(1):33-44. doi: 10.1177/1759720X12468659. Ther Adv Musculoskelet Dis. 2013. PMID: 23515070 Free PMC article.
-
Pharmacological inhibition of Peroxisome Proliferation-Activated Receptor Delta (PPARδ) imparts selective leukemia cell death.Cancer Metab. 2025 Jul 25;13(1):36. doi: 10.1186/s40170-025-00402-5. Cancer Metab. 2025. PMID: 40713763 Free PMC article.
-
Potential benefits of green tea polyphenol EGCG in the prevention and treatment of vascular inflammation in rheumatoid arthritis.Life Sci. 2013 Sep 3;93(8):307-12. doi: 10.1016/j.lfs.2013.07.006. Epub 2013 Jul 19. Life Sci. 2013. PMID: 23871988 Free PMC article. Review.
-
Successful treatment of xanthoma disseminatum with combined lipid lowering agents.Ann Dermatol. 2012 Aug;24(3):380-2. doi: 10.5021/ad.2012.24.3.380. Epub 2012 Jul 25. Ann Dermatol. 2012. PMID: 22879732 Free PMC article. No abstract available.
References
-
- Castelli WP, Garrison RJ, Wilson PWF, et al. Incidence of coronary heart disease and lipoprotein cholesterol levels: The Framingham Study. JAMA. 1986;256:2835–2838. - PubMed
-
- Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults Executive Summary of the Third Report of the National Cholesterol Education Program (Adult Treatment Panel III) JAMA. 2001;285:2486–2497. - PubMed
-
- Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation. 2002;106:3143–3421. - PubMed
-
- Cannon CP, Braunwald E, McCabe CH, et al. Intensive versus moderate lipid lowering with statins after acute coronary syndromes. N Engl J Med. 2004;350:1495–1504. - PubMed
-
- LaRosa JC, Grundy SM, Waters DD, et al. Intensive lipid lowering with atorvastatin in patients with stable coronary disease. N Engl J Med. 2005;352:1425–1435. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
