

Increased postprandial nonesterified fatty acid appearance and oxidation in type 2 diabetes is not fully established in offspring of diabetic subjects
- PMID: 20532041
- PMCID: PMC2881041
- DOI: 10.1371/journal.pone.0010956
Increased postprandial nonesterified fatty acid appearance and oxidation in type 2 diabetes is not fully established in offspring of diabetic subjects
Abstract
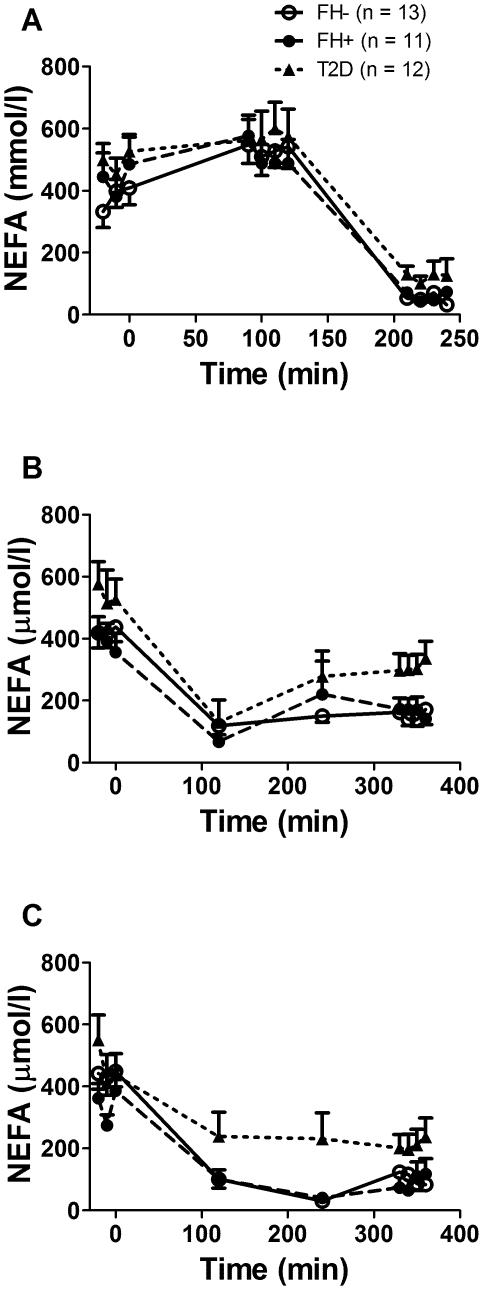
Background: It has been proposed that abnormal postprandial plasma nonesterified fatty acid (NEFA) metabolism may participate in the development of tissue lipotoxicity and type 2 diabetes (T2D). We previously found that non-diabetic offspring of two parents with T2D display increased plasma NEFA appearance and oxidation rates during intravenous administration of a fat emulsion. However, it is currently unknown whether plasma NEFA appearance and oxidation are abnormal during the postprandial state in these subjects at high-risk of developing T2D.
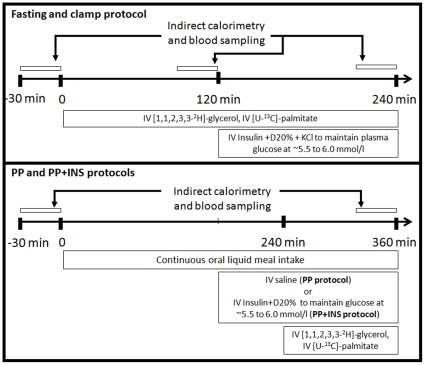
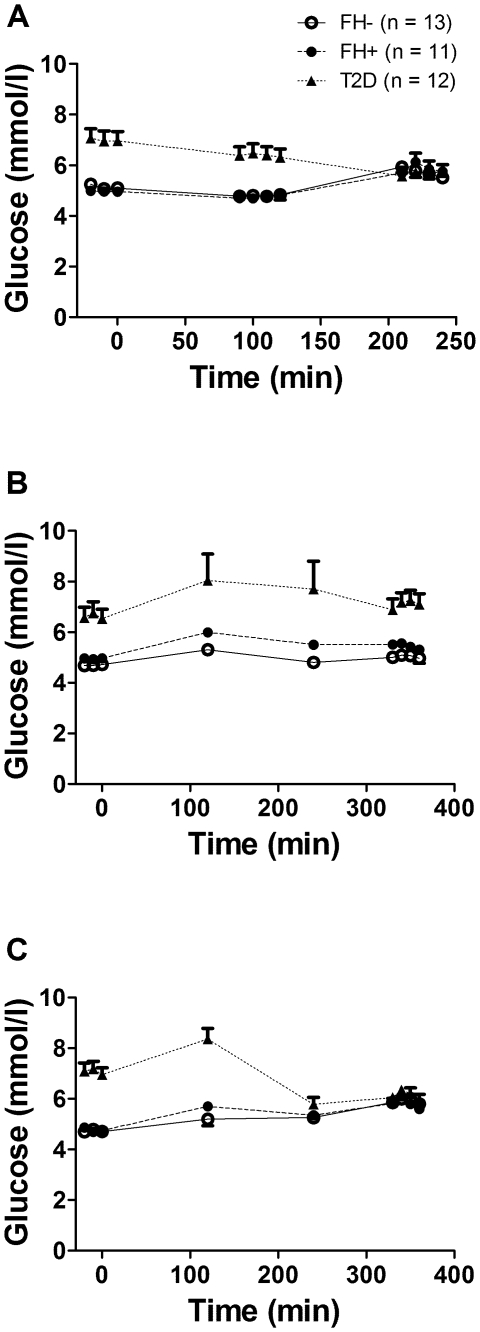
Methodology: Palmitate appearance and oxidation rates and glycerol appearance rate were determined in eleven healthy offspring of two parents with T2D (positive family history, FH+), 13 healthy subjects without first-degree relatives with T2D (FH-) and 12 subjects with T2D at fasting, during normoglycemic hyperinsulinemic clamp and during continuous oral intake of a standard liquid meal to achieve steady postprandial NEFA and triacylglycerols (TG) without and with insulin infusion to maintain similar glycemia in all three groups.
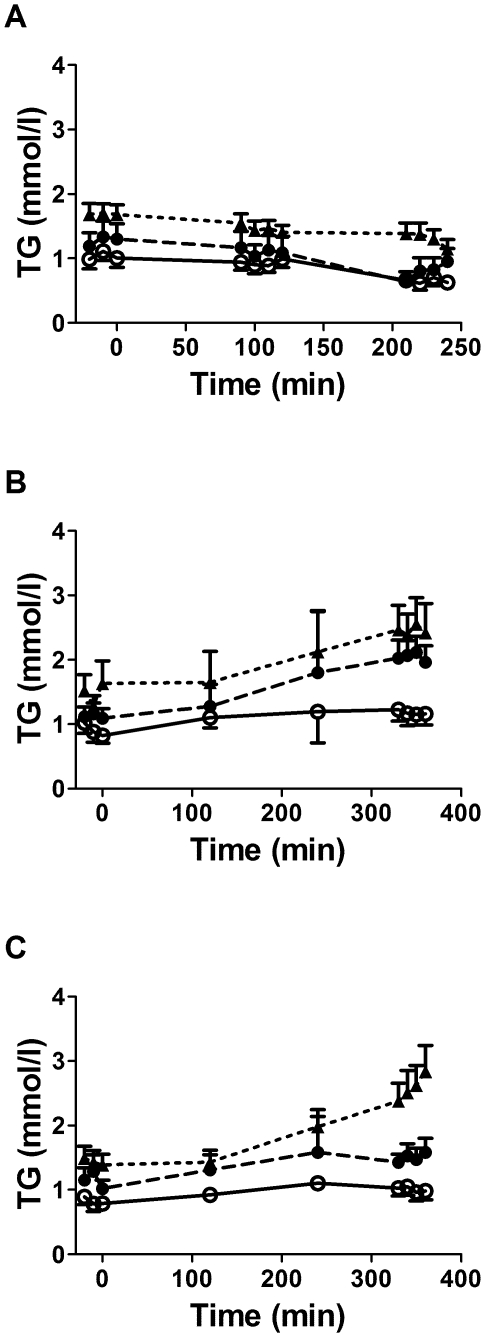
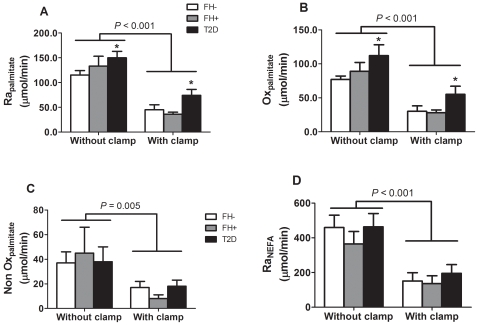
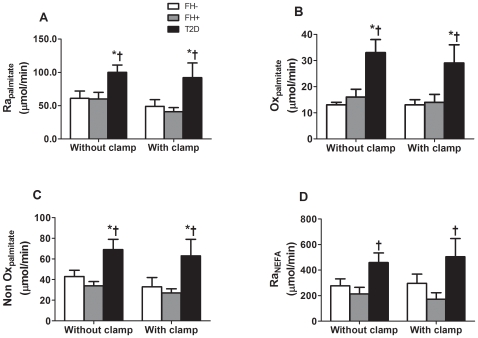
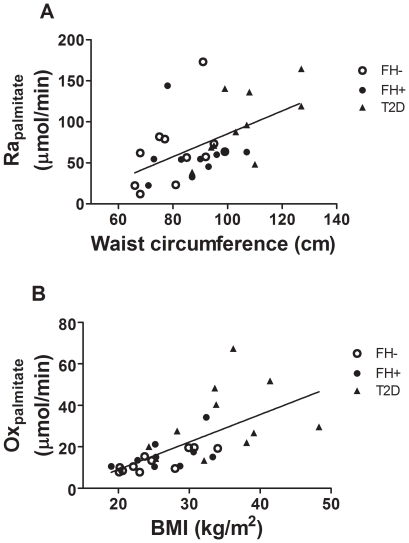
Principal findings: Plasma palmitate appearance and oxidation were higher at fasting and during the clamp conditions in the T2D group (all P<0.05). In the postprandial state, palmitate appearance, oxidative and non oxidative rates were all elevated in T2D (all P<0.05) but not in FH+. Both T2D and FH+ displayed elevated postprandial TG vs. FH- (P<0.001). Acute correction of hyperglycemia during the postprandial state did not affect these group differences. Increased waist circumference and BMI were positively associated with elevated postprandial plasma palmitate appearance and oxidation.
Conclusions/significance: Postprandial plasma NEFA intolerance observed in subjects with T2D is not fully established in non-diabetic offspring of both parents with T2D, despite the presence of increased postprandial plasma TG in the later. Elevated postprandial plasma NEFA appearance and oxidation in T2D is observed despite acute correction of the exaggerated glycemic excursion in this group.
Conflict of interest statement
Figures
References
-
- Martin BC, Warram JH, Krolewski AS, Bergman RN, Soeldner JS, et al. Role of glucose and insulin resistance in development of type 2 diabetes mellitus: results of a 25-year follow-up study [see comments]. Lancet. 1992;340:925–929. - PubMed
-
- Axelsen M, Smith U, Eriksson JW, Taskinen MR, Jansson PA. Postprandial hypertriglyceridemia and insulin resistance in normoglycemic first-degree relatives of patients with type 2 diabetes. Annals of Internal Medicine. 1999;131:27–31. - PubMed
-
- Lewis GF, Carpentier A, Adeli K, Giacca A. Disordered fat storage and mobilization in the pathogenesis of insulin resistance and type 2 diabetes. Endocr Rev. 2002;23:201–229. - PubMed
-
- Lavoie F, Frisch F, Brassard P, Normand-Lauziere F, Cyr D, et al. Relationship between Total and High Molecular Weight Adiponectin Levels and Plasma Nonesterified Fatty Acid Tolerance during Enhanced Intravascular Triacylglycerol Lipolysis in Men. J Clin Endocrinol Metab. 2009;94:998–1004. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
