

The surgical treatment of hepatic metastases in colorectal carcinoma
- PMID: 20532128
- PMCID: PMC2881614
- DOI: 10.3238/arztebl.2010.0335
The surgical treatment of hepatic metastases in colorectal carcinoma
Abstract
Background: Colorectal carcinoma with hepatic metastases was long considered an incurable disease. Recent advances in surgical treatment have substantially improved the affected patients' prognosis. At first, surgery was only performed in patients whose hepatic tumor burden was small (<4 nodes, <5 cm). Currently, however, the main issue is the feasibility of curative resection of all metastases.
Method: The PubMed literature database was selectively searched for articles with the keywords "colorectal liver metastases," "chemotherapy," and "surgery." Particular attention was devoted to studies of large groups of patients, randomized trials, the German guidelines, and an analysis of the authors' own patient population.
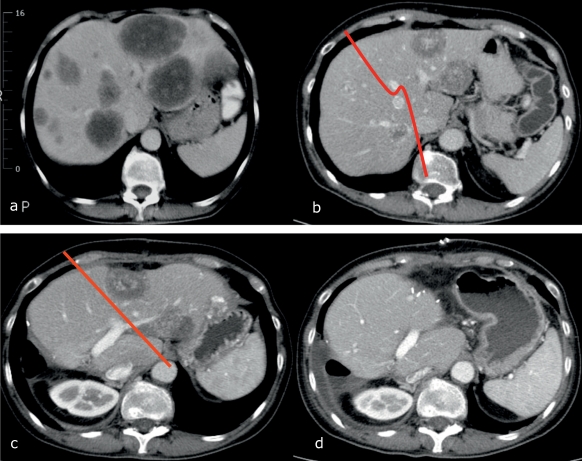
Results: Only 10% to 20% of all patients are candidates for surgical therapy (hepatic resection), as the rest are disqualified either by extensive liver involvement or by extrahepatic neoplasia. A further 10% of patients have hepatic metastases that are primarily considered inoperable, yet later become amenable to surgery after interdisciplinary treatment involving preoperative chemotherapy, portal-vein embolization, two-stage hepatectomy, and/or locally ablative procedures. Chemotherapy is probably beneficial after hepatic resection, although the benefit has not yet been definitively demonstrated by clinical trials. Therefore, chemotherapy should only be given perioperatively in selected cases, when recommended by an interdisciplinary treatment team.
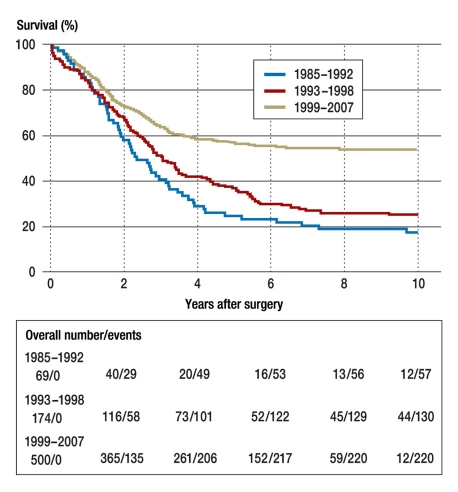
Conclusion: A multimodal approach to the treatment of hepatic metastases of colorectal carcinoma has led to an increase in the number of resections and to an improved long-term survival rate (currently more than 40% at 5 years).
Figures
Similar articles
-
[Diagnosis and treatment of colorectal liver metastases - workflow].Zentralbl Chir. 2008 Jun;133(3):267-84. doi: 10.1055/s-2008-1076796. Zentralbl Chir. 2008. PMID: 18563694 Review. German.
-
Combined first-stage hepatectomy and colorectal resection in a two-stage hepatectomy strategy for bilobar synchronous liver metastases.Br J Surg. 2010 Sep;97(9):1354-62. doi: 10.1002/bjs.7128. Br J Surg. 2010. PMID: 20603857
-
[Colorectal liver metastases. Neoadjuvant chemotherapy: aspects of medical and surgical oncology].Internist (Berl). 2007 Jan;48(1):51-8. doi: 10.1007/s00108-006-1770-0. Internist (Berl). 2007. PMID: 17160665 Review. German.
-
[Colorectal cancer liver metastases -- neoadjuvant concepts for preoperative down-sizing].Zentralbl Chir. 2006 Apr;131(2):140-7. doi: 10.1055/s-2006-921538. Zentralbl Chir. 2006. PMID: 16612781 Review. German.
-
Results of surgical treatment for multiple (> or =5 nodules) bi-lobar hepatic metastases from colorectal cancer.Langenbecks Arch Surg. 2004 Apr;389(2):114-21. doi: 10.1007/s00423-003-0447-6. Epub 2004 Jan 9. Langenbecks Arch Surg. 2004. PMID: 14714186
Cited by
-
The evolution of cancer surgery and future perspectives.Nat Rev Clin Oncol. 2015 Feb;12(2):115-24. doi: 10.1038/nrclinonc.2014.191. Epub 2014 Nov 11. Nat Rev Clin Oncol. 2015. PMID: 25384943 Review.
-
Robotic Stereotactic Body Radiation Therapy for Oligometastatic Liver Metastases: A Systematic Review of the Literature and Evidence Quality Assessment.Diagnostics (Basel). 2024 May 19;14(10):1055. doi: 10.3390/diagnostics14101055. Diagnostics (Basel). 2024. PMID: 38786353 Free PMC article. Review.
-
Iron Oxide Nanoparticle-Based Hyperthermia as a Treatment Option in Various Gastrointestinal Malignancies.Nanomaterials (Basel). 2021 Nov 10;11(11):3013. doi: 10.3390/nano11113013. Nanomaterials (Basel). 2021. PMID: 34835777 Free PMC article. Review.
-
[Preoperative imaging/operation planning for liver surgery].Chirurg. 2015 Dec;86(12):1167-79; quiz 1180-1. doi: 10.1007/s00104-015-0107-8. Chirurg. 2015. PMID: 26606924 Review. German.
-
Current state of surgical treatment of liver metastases from colorectal cancer.World J Gastrointest Surg. 2011 Dec 27;3(12):183-96. doi: 10.4240/wjgs.v3.i12.183. World J Gastrointest Surg. 2011. PMID: 22224173 Free PMC article.
References
-
- Scheele J, Stangl R, Altendorf-Hofmann A. Hepatic metastases from colorectal carcinoma: impact of surgical resection on the natural history. Br J Surg. 1990;77:1241–1246. - PubMed
-
- Jonas S, Thelen A, Benckert C, et al. Extended resections of liver metastases from colorectal cancer. World J Surg. 2007;31:511–521. - PubMed
-
- Folprecht G, Grothey A, Alberts S, Raab HR, Kohne CH. Neoadjuvant treatment of unresectable colorectal liver metastases: correlation between tumour response and resection rates. Ann Oncol. 2005;16:1311–1319. - PubMed
-
- Fernandez FG, Drebin JA, Linehan DC, Dehdashti F, Siegel BA, Strasberg SM. Five-year survival after resection of hepatic metas-tases from colorectal cancer in patients screened by positron emission tomography with F-18 fluorodeoxyglucose (FDG-PET) Ann Surg. 2004;240:438–447. 447–450. discussion. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical