

Medication adherence, self-care behaviour and knowledge on heart failure in urban South Africa: the Heart of Soweto study
- PMID: 20532432
- PMCID: PMC3721814
Medication adherence, self-care behaviour and knowledge on heart failure in urban South Africa: the Heart of Soweto study
Abstract
Background: There is a paucity of data on treatment adherence in patients with chronic heart failure (CHF) in Africa.
Methods: We examined the pattern of treatment adherence, self-care behaviour and treatment knowledge in 200 consecutive patients with CHF attending the Chris Hani Baragwanath Hospital, Soweto, South Africa via a combination of questionnaire (100%, n = 200) and pill count (41%, n = 82).
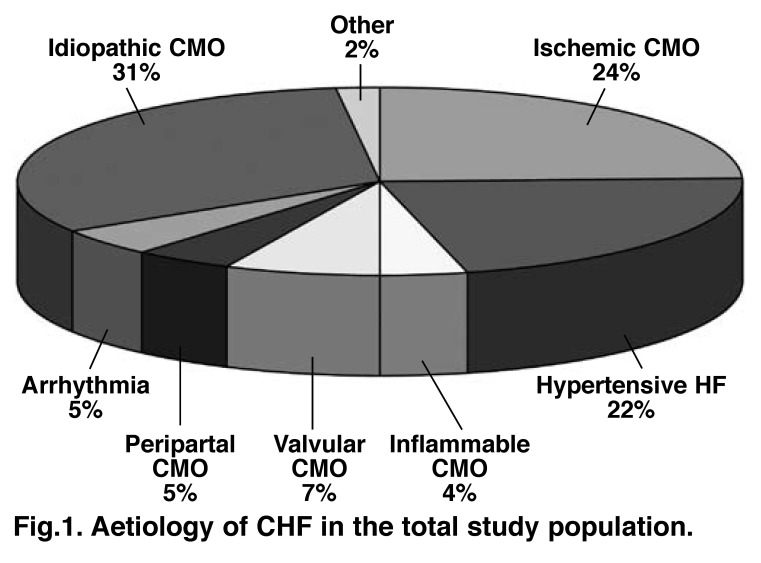
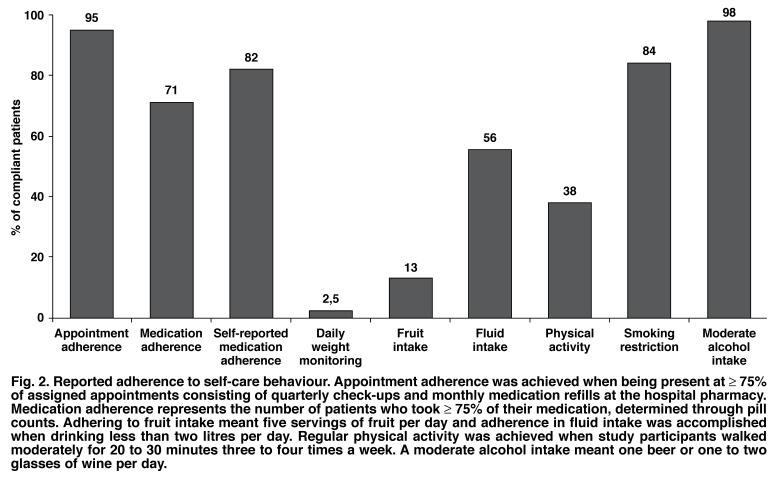
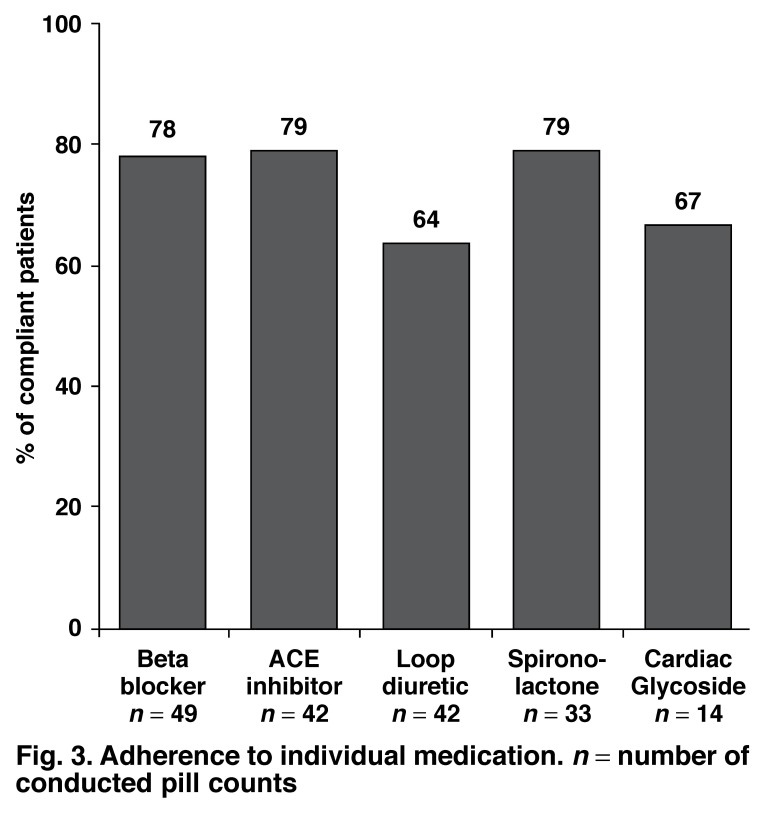
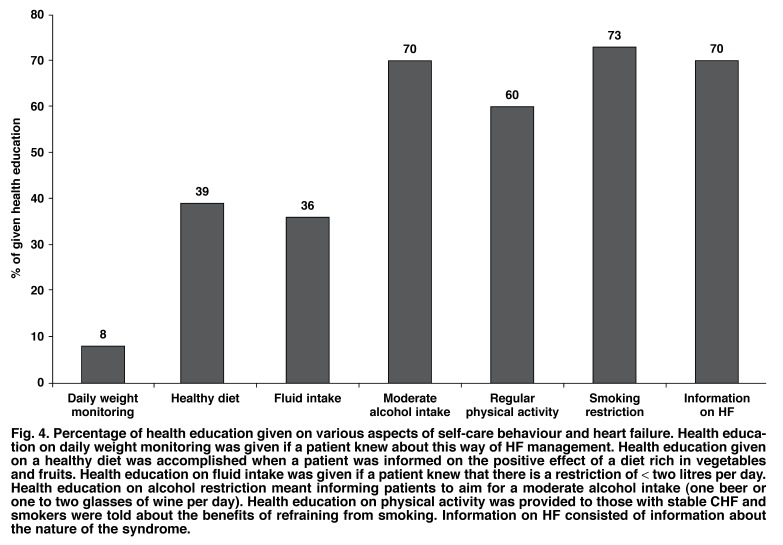
Results: Mean age was 56 +/- 14 years, 157 were black African (79%) and 109 (55%) were male. CHF-specific treatment included loop diuretics (93%), beta-blockers (84%), ACE inhibitors (74%), spironolactone (64%) and cardiac glycosides (24%); mean number of medications was 6 +/- 2. Overall, 71% (58 of 82) adhered to their prescribed CHF regimen and individual medication adherence ranged from 64 to 79%. Behavioural adherence varied from 2.5 to 98%. Patient treatment knowledge was poor; 56% could not name medication effects or side effects. However, an average knowledge score of 69% was achieved on 10 questions concerning CHF management.
Conclusion: As in other regions of the world, non-adherence to complex CHF treatment is a substantial problem in Soweto. Our data confirm the need for a dedicated CHF management programme to optimise CHF-related outcomes in a low-resource environment.
Figures
References
-
- Sliwa K, Damasceno A, Mayosi B. Epidemiology and etiology of cardiomyopathy in Africa. Circulation. 2005;112:3577–3583. - PubMed
-
- Stewart S, Wilkinson D, Becker A. et al. Mapping the emergence of heart disease in a black urban population in Africa: The Heart of Soweto Study. Int J Cardiol. 2006;101:101–108. - PubMed
-
- Damesceno A, Cotter G, Sliwa K, Mayosi BM. Heart failure in sub-Saharan Africa: Time for Action. J Am Coll Cardiol. 2007;50:1688–1693. - PubMed
-
- Inglis SC, Stewart S, Papachan A. et al. Anaemia and renal function in heart failure due to idiopathic dilated cardiomyopathy. Eur J Heart Fail. 2007;9:384–390. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
