

Adherence to osteoporosis drugs and fracture prevention: no evidence of healthy adherer bias in a frail cohort of seniors
- PMID: 20532481
- PMCID: PMC3277855
- DOI: 10.1007/s00198-010-1309-z
Adherence to osteoporosis drugs and fracture prevention: no evidence of healthy adherer bias in a frail cohort of seniors
Abstract
We examined new users of osteoporosis drugs among seniors in Pennsylvania and found no evidence of healthy adherer bias on observed associations between adherence to treatment and non-vertebral fracture risk; we document fracture reduction with better adherence to bisphosphonates, yet no fracture reduction with better adherence to calcitonin or raloxifene.
Introduction: We examined the potential for "healthy adherer bias" when studying the effects of adherence to osteoporosis pharmacotherapy on fracture risk. Based on clinical trial evidence, bisphosphonates, calcitonin, and raloxifene reduce vertebral fracture risk; yet only bisphosphonates are documented to reduce non-vertebral fracture risk.
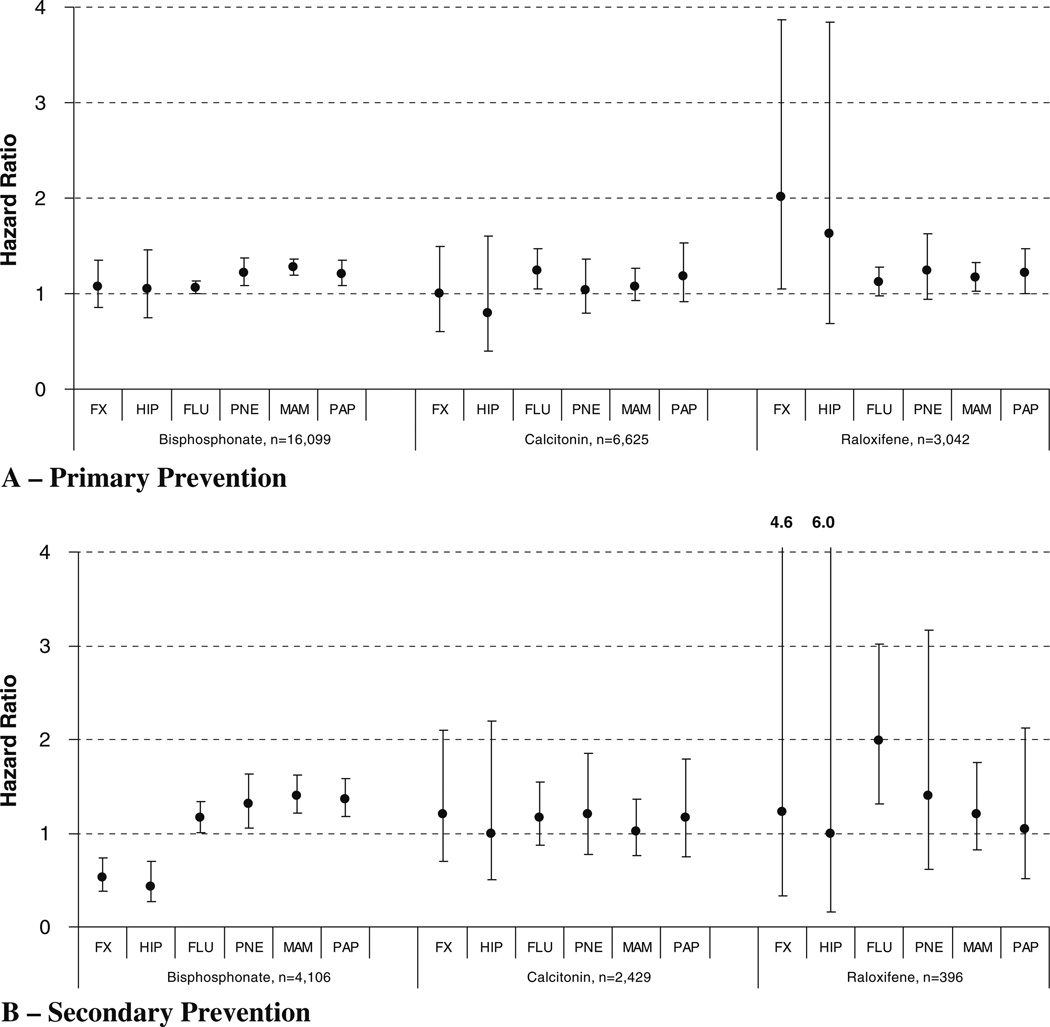
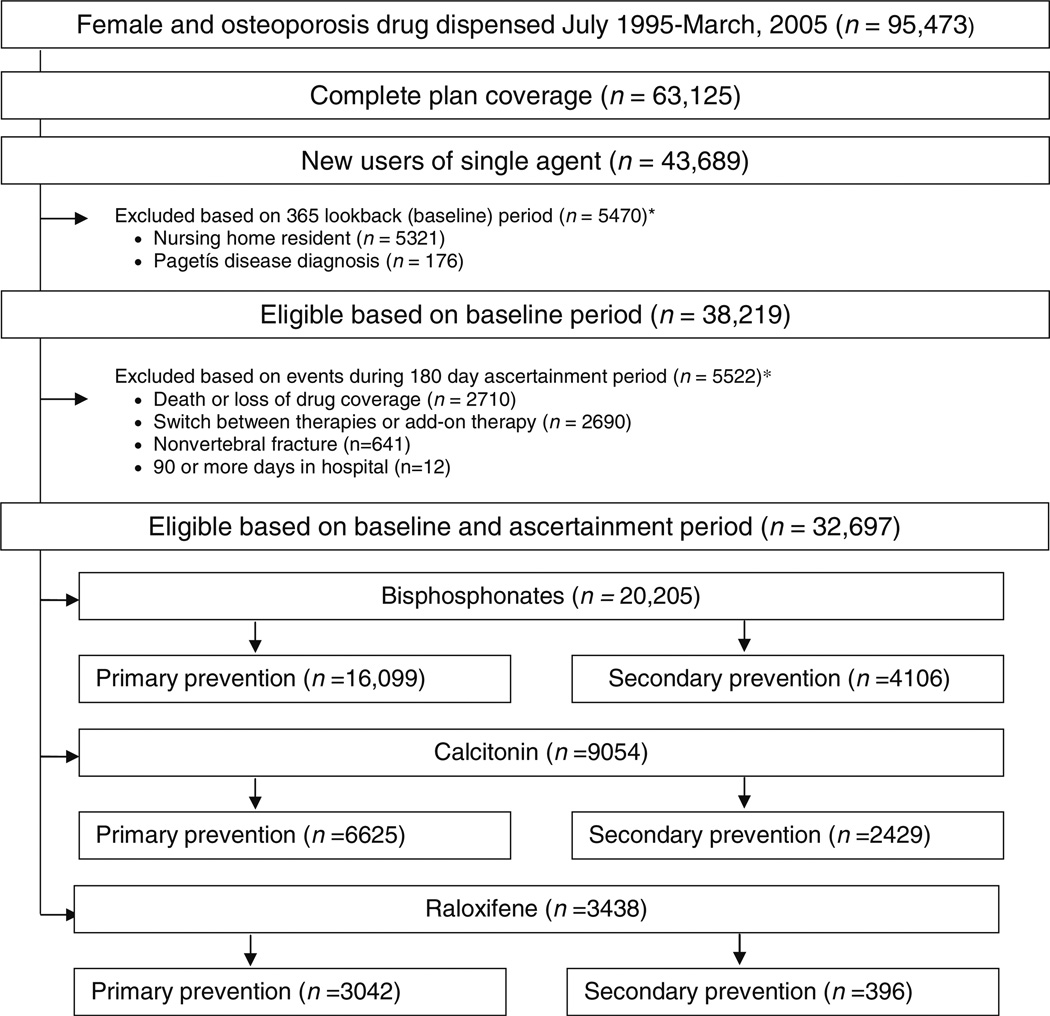
Methods: This is a cohort study of older women in Pennsylvania who initiated osteoporosis drugs between 1995 and 2005. We included new users of bisphosphonates, calcitonin, and raloxifene. Adherence was categorized based on a measure of compliance as high [proportion of days covered (PDC) ≥ 80%], intermediate (50% < PDC < 80%), or low (PDC ≤ 50%) according to a 180-day ascertainment period. Non-vertebral fracture rates within 365 days after the ascertainment period were compared between adherence categories (reference = low) using Cox proportional hazard models and adjusting for fracture risk factors. Primary and secondary prevention cohorts were examined separately. Adherence to calcitonin and raloxifene were control analyses.
Results: We found little difference in fracture rates between levels of adherence to calcitonin, bisphosphonates for primary prevention, or raloxifene for secondary prevention. We document lower fracture rates among high versus low adherent bisphosphonate users for secondary prevention (HR = 0.53, 95%CI = 0.38-0.74) and higher fracture rates among high versus low adherent raloxifene users for primary prevention (HR = 2.01, 95%CI = 1.04-3.87).
Conclusions: We document little evidence of healthy adherer bias when studying the association between better adherence to osteoporosis drugs and fracture risk reduction, with only better adherence to bisphosphonates reducing fracture risk. The higher fracture risk among highly adherent raloxifene users for primary prevention is likely due to residual confounding.
Conflict of interest statement
Figures

Similar articles
-
Comparative effectiveness of osteoporosis drugs in preventing secondary nonvertebral fractures in Taiwanese women.J Clin Endocrinol Metab. 2013 Dec;98(12):4717-26. doi: 10.1210/jc.2013-1877. Epub 2013 Sep 30. J Clin Endocrinol Metab. 2013. PMID: 24081731
-
Relative effectiveness of osteoporosis drugs for preventing nonvertebral fracture.Ann Intern Med. 2008 May 6;148(9):637-46. doi: 10.7326/0003-4819-148-9-200805060-00003. Ann Intern Med. 2008. PMID: 18458276 Free PMC article.
-
Denosumab, raloxifene, romosozumab and teriparatide to prevent osteoporotic fragility fractures: a systematic review and economic evaluation.Health Technol Assess. 2020 Jun;24(29):1-314. doi: 10.3310/hta24290. Health Technol Assess. 2020. PMID: 32588816 Free PMC article.
-
Effect of Bisphosphonates on Fracture Outcomes Among Frail Older Adults.J Am Geriatr Soc. 2019 Apr;67(4):768-776. doi: 10.1111/jgs.15725. Epub 2018 Dec 21. J Am Geriatr Soc. 2019. PMID: 30575958 Free PMC article.
-
Medical treatment of vertebral osteoporosis.Eur Spine J. 2003 Oct;12 Suppl 2(Suppl 2):S132-41. doi: 10.1007/s00586-003-0608-x. Epub 2003 Sep 17. Eur Spine J. 2003. PMID: 13680313 Free PMC article. Review.
Cited by
-
Improving adherence to and persistence with oral therapy of osteoporosis.Osteoporos Int. 2015 May;26(5):1629-38. doi: 10.1007/s00198-015-3038-9. Epub 2015 Jan 27. Osteoporos Int. 2015. PMID: 25619634 Clinical Trial.
-
The complex relation between bisphosphonate adherence and fracture reduction.J Clin Endocrinol Metab. 2010 Jul;95(7):3251-9. doi: 10.1210/jc.2009-2778. Epub 2010 May 5. J Clin Endocrinol Metab. 2010. PMID: 20444916 Free PMC article.
-
Association between teriparatide adherence and healthcare utilization and costs in real-world US kyphoplasty/vertebroplasty patients.Osteoporos Int. 2013 Sep;24(9):2525-33. doi: 10.1007/s00198-013-2324-7. Epub 2013 Mar 26. Osteoporos Int. 2013. PMID: 23529293
-
Real-world persistence and adherence with oral bisphosphonates for osteoporosis: a systematic review.BMJ Open. 2019 Apr 14;9(4):e027049. doi: 10.1136/bmjopen-2018-027049. BMJ Open. 2019. PMID: 30987990 Free PMC article.
-
Methods to examine the impact of compliance to osteoporosis pharmacotherapy on fracture risk: systematic review and recommendations.Ther Adv Chronic Dis. 2010 Nov 1;1(4):149-162. doi: 10.1177/2040622310376137. Ther Adv Chronic Dis. 2010. PMID: 22282723 Free PMC article.
References
-
- Burge R, Dawson-Hughes B, Solomon DH, et al. Incidence and economic burden of osteoporosis-related fractures in the United States, 2005–2025. J Bone Miner Res. 2007;22:465–475. - PubMed
-
- MacLean C, Newberry S, Maglione M, et al. Systematic review: comparative effectiveness of treatments to prevent fractures in men and women with low bone density or osteoporosis. Ann Intern Med. 2008;148:197–213. - PubMed
-
- Kothawala P, Badamgarav E, Ryu S, et al. Systematic review and meta-analysis of real-world adherence to drug therapy for osteoporosis. Mayo Clin Proc. 2007;82:1493–1501. - PubMed
-
- Siris ES, Selby PL, Saag KG, et al. Impact of osteoporosis treatment adherence on fracture rates in North America and Europe. Am J Med. 2009;122:S3–S13. - PubMed
-
- Wilkes MM, Navickis RJ, Chan WW, et al. Bisphosphonates and osteoporotic fractures: a cross-design synthesis of results among compliant/persistent postmenopausal women in clinical practice versus randomized controlled trials. Osteoporos Int. 2010;21:679–688. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
