

In situ pinning with arthroscopic osteoplasty for mild SCFE: A preliminary technical report
- PMID: 20532715
- PMCID: PMC2974872
- DOI: 10.1007/s11999-010-1408-3
In situ pinning with arthroscopic osteoplasty for mild SCFE: A preliminary technical report
Abstract
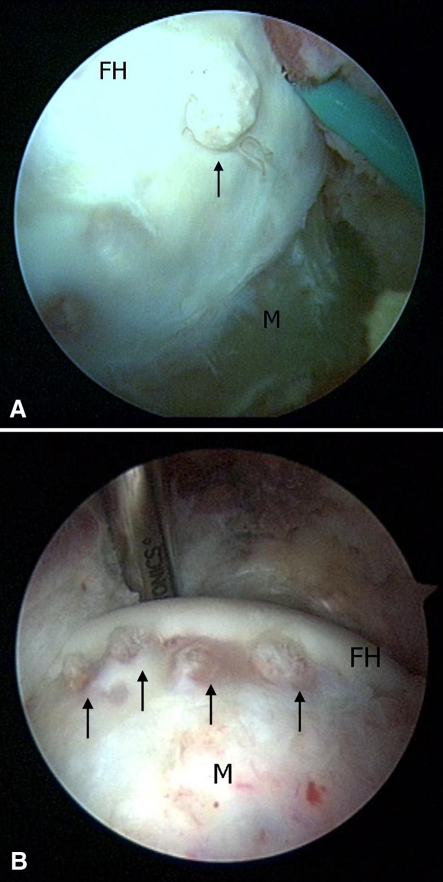
Background: There is emerging evidence that even mild slipped capital femoral epiphysis leads to early articular damage. Therefore, we have begun treating patients with mild slips and signs of impingement with in situ pinning and immediate arthroscopic osteoplasty. DESCRIPTION OF TECHNIQUES: Surgery was performed using the fracture table. After in situ pinning and diagnostic arthroscopy, peripheral compartment access was obtained and head-neck osteoplasty was completed.
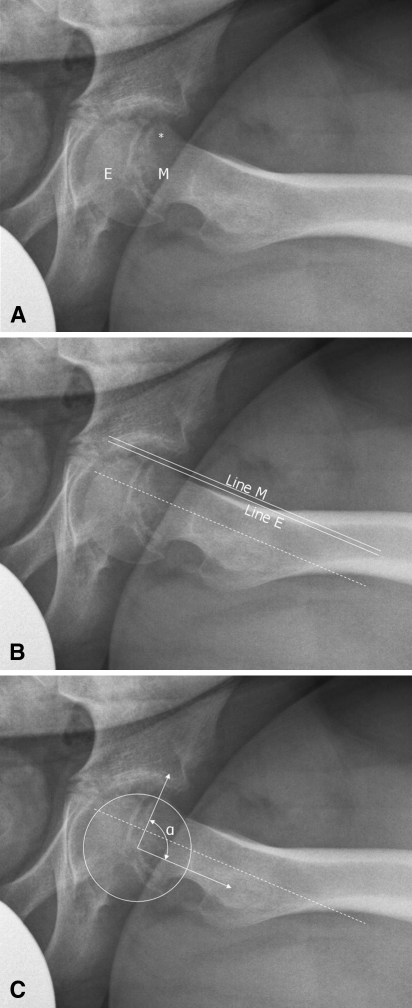
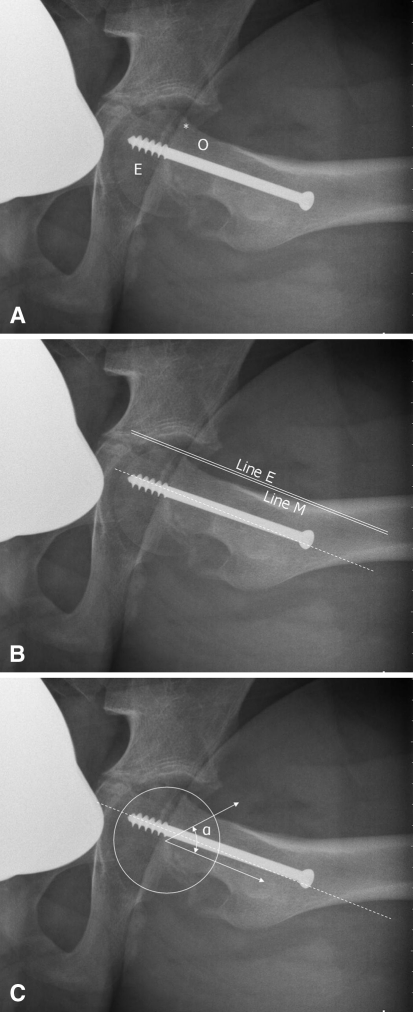
Methods: Between March 2008 and August 2009, three male patients (age range, 11-15 years; BMI, 22-31 kg/m(2)) presented with slip angles between 15º and 30º. All were ambulatory without assistance but had 2 to 12 weeks of hip and/or knee pain, limited motion and a positive impingement test. Postoperatively, patients were assessed at 6 weeks; 3 and 6 months; then every 6 months for the first two years. Hip motion, epiphyseal-metaphyseal offsets and alpha angles were determined. Patients completed the UCLA activity scale at latest followup that ranged from 6 to 23 months.
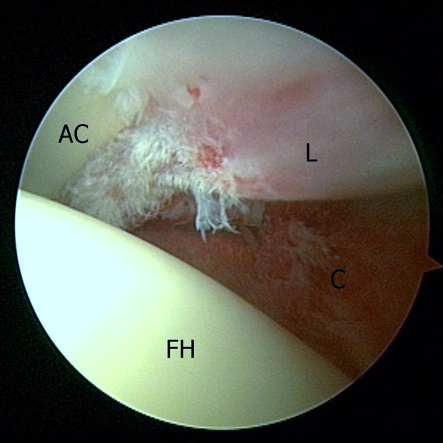
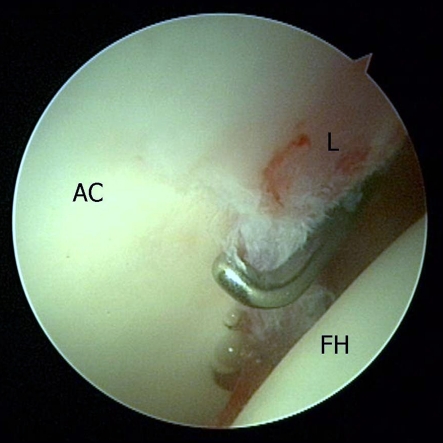
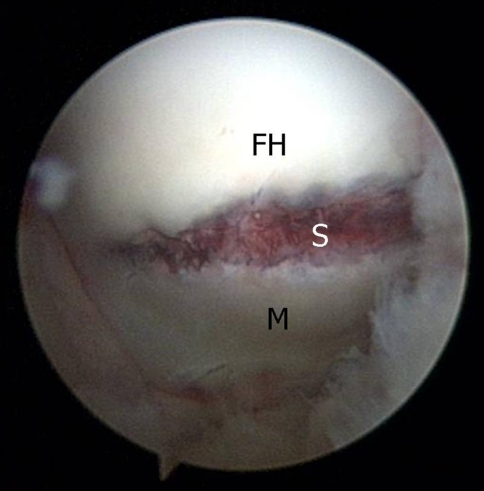
Results: Arthroscopic evaluation revealed labral fraying, acetabular chondromalacia, and a prominent metaphyseal ridge. At last followup, each was pain-free and had returned to unrestricted activities. Hip motion improved in all and none demonstrated clinical impingement. Radiographs showed normalized epiphyseal-metaphyseal offsets and alpha angles.
Conclusions: In situ pinning with arthroscopic osteoplasty can limit impingement after mild slipped capital femoral epiphysis. Due to limited followup, we are unable to say whether this protocol reduces subsequent articular damage. Although we recommend performing these procedures concomitantly, they can be performed in a staged fashion, especially since hip arthroscopy following an epiphyseal slip can be challenging.
Figures

References
-
- Amstutz HC, Thomas BJ, Jinnah R, Kim W, Grogan T, Yale C. Treatment of primary osteoarthritis of the hip. A comparison of total joint and surface replacement arthroplasty. J Bone Joint Surg Am. 1984;66:228–241. - PubMed
-
- Aronsson DD, Loder RT, Breur GJ, Weinstein SL. Slipped capital femoral epiphysis: current concepts. J Am Acad Orthop Surg. 2006;14:666–679. - PubMed
-
- Boyer DW, Mickelson MR, Ponseti IV. Slipped capital femoral epiphysis. Long-term follow-up study of one hundred and twenty-one patients. J Bone Joint Surg Am. 1981;63:85–95. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
