

Reduction of the closure time of postoperative enterocutaneous fistulas with fibrin sealant
- PMID: 20533600
- PMCID: PMC2883136
- DOI: 10.3748/wjg.v16.i22.2793
Reduction of the closure time of postoperative enterocutaneous fistulas with fibrin sealant
Abstract
Aim: To assess whether the use of fibrin sealant shortens the closure time of postoperative enterocutaneous fistulas (ECFs).
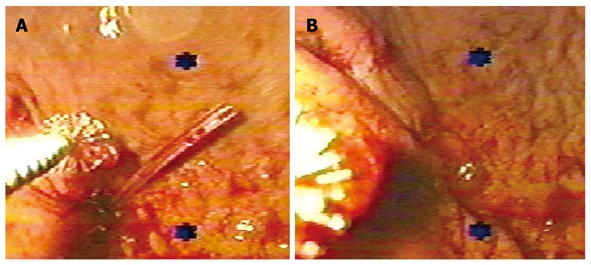
Methods: The prospective case-control study included 70 patients with postoperative ECFs with an output of < 500 mL/d, a fistulous tract of > 2 cm and without any local complication. They were divided into study (n = 23) and control groups (n = 47). Esophageal, gastric and colocutaneous fistulas were monitored under endoscopic visualization, which also allowed fibrin glue application directly through the external hole. Outcome variables included closure time, time to resume oral feeding and morbidity related to nutritional support.
Results: There were no differences in mean age, fistula output, and follow-up. Closure-time for all patients of the study group was 12.5 +/- 14.2 d and 32.5 +/- 17.9 d for the control group (P < 0.001), and morbidity related to nutritional support was 8.6% and 42.5%, respectively (P < 0.01). In patients with colonic fistulas, complete closure occurred 23.5 +/- 19.5 d after the first application of fibrin glue, and spontaneous closure was observed after 36.2 +/- 22.8 d in the control group (P = 0.36). Recurrences were observed in 2 patients because of residual disease. One patient of each group died during follow-up as a consequence of septic complications related to parenteral nutrition.
Conclusion: Closure time was significantly reduced with the use of fibrin sealant, and oral feeding was resumed faster. We suggest the use of fibrin sealant for the management of stable enterocutaneous fistulas.
Figures
References
-
- Berry SM, Fischer JE. Classification and pathophysiology of enterocutaneous fistulas. Surg Clin North Am. 1996;76:1009–1018. - PubMed
-
- Arenas-Marquez H, Anaya-Prado R, Hurtado H, Juarez F, Fernandez J, Galindo-Mendoza L, Terrazas-Espitia F, Aiello V, Mondragón R, Gudiño-Lever I, et al. Mexican consensus on the integral management of digestive tract fistulas. Ixtapa-Zihuatanejo, Mexico, August 21-23, 1997. Nutrition. 1999;15:235–238. - PubMed
-
- Metcalf C. Enterocutaneous fistulae. J Wound Care. 1999;8:141–142. - PubMed
-
- Berry SM, Fischer JE. Enterocutaneous fistulas. Curr Probl Surg. 1994;31:469–566. - PubMed
-
- Evenson AR, Fischer JE. Current management of enterocutaneous fistula. J Gastrointest Surg. 2006;10:455–464. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
