

Survival trends in critically ill HIV-infected patients in the highly active antiretroviral therapy era
- PMID: 20534139
- PMCID: PMC2911753
- DOI: 10.1186/cc9056
Survival trends in critically ill HIV-infected patients in the highly active antiretroviral therapy era
Abstract
Introduction: The widespread use of highly active antiretroviral therapy (ART) has reduced HIV-related life-threatening infectious complications. Our objective was to assess whether highly active ART was associated with improved survival in critically ill HIV-infected patients.
Methods: A retrospective study from 1996 to 2005 was performed in a medical intensive care unit (ICU) in a university hospital specialized in the management of immunocompromised patients. A total of 284 critically ill HIV-infected patients were included. Differences were sought across four time periods. Risk factors for death were identified by multivariable logistic regression.
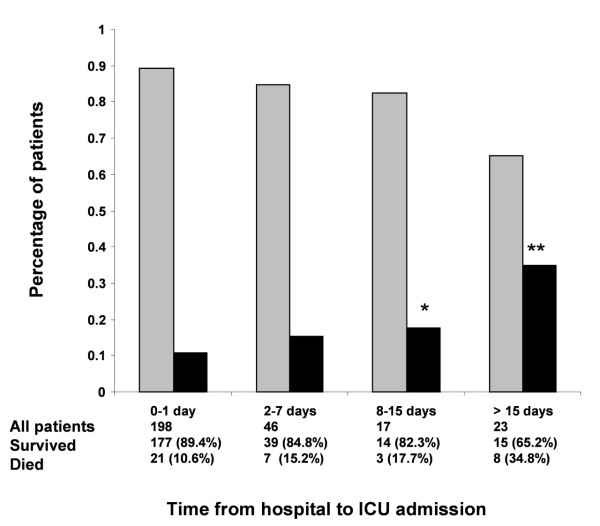
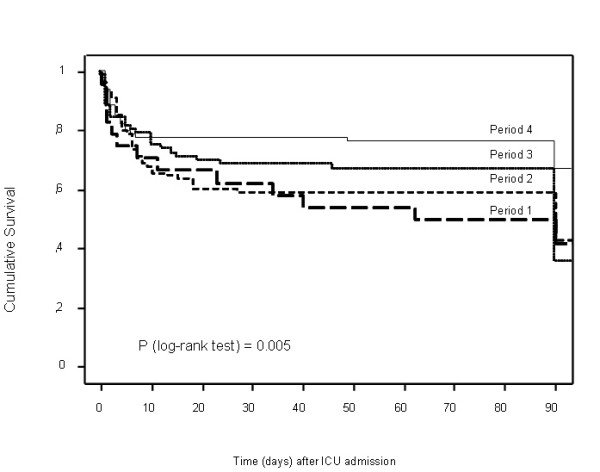
Results: Among the 233 (82%) patients with known HIV infection before ICU admission, 64% were on highly active ART. Annual admissions increased over time, with no differences in reasons for admission: proportions of patients with newly diagnosed HIV, previous opportunistic infection, CD4 counts, viral load, or acute disease severity. ICU and 90-day mortality rates decreased steadily: 25% and 37.5% in 1996 to 1997, 17.1% and 17.1% in 1998 to 2000, 13.2% and 13.2% in 2001 to 2003, and 8.6% in 2004 to 2005. Five factors were independently associated with increased ICU mortality: delayed ICU admission (odds ratio (OR), 3.04; 95% confidence interval (CI), 1.29 to 7.17), acute renal failure (OR, 4.21; 95% CI, 1.63 to 10.92), hepatic cirrhosis (OR, 3.78; 95% CI, 1.21 to 11.84), ICU admission for coma (OR, 2.73; 95% CI, 1.16 to 6.46), and severe sepsis (OR, 3.67; 95% CI, 1.53 to 8.80). Admission to the ICU in the most recent period was independently associated with increased survival: admission from 2001 to 2003 (OR, 0.28; 95% CI, 0.08 to 0.99), and between 2004 and 2005 (OR, 0.13; 95% CI, 0.03 to 0.53).
Conclusions: ICU survival increased significantly in the highly active ART era, although disease severity remained unchanged. Co-morbidities and organ dysfunctions, but not HIV-related variables, were associated with death. Earlier ICU admission from the hospital ward might improve survival.
Figures
References
-
- Palella FJ, Delaney KM, Moorman AC, Loveless MO, Fuhrer J, Satten GA, Aschman DJ, Holmberg SD. Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. HIV Outpatient Study Investigators. N Engl J Med. 1998;338:853–860. doi: 10.1056/NEJM199803263381301. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
