

A pharmacodynamic study of sorafenib in patients with relapsed and refractory acute leukemias
- PMID: 20535150
- PMCID: PMC2921005
- DOI: 10.1038/leu.2010.132
A pharmacodynamic study of sorafenib in patients with relapsed and refractory acute leukemias
Abstract
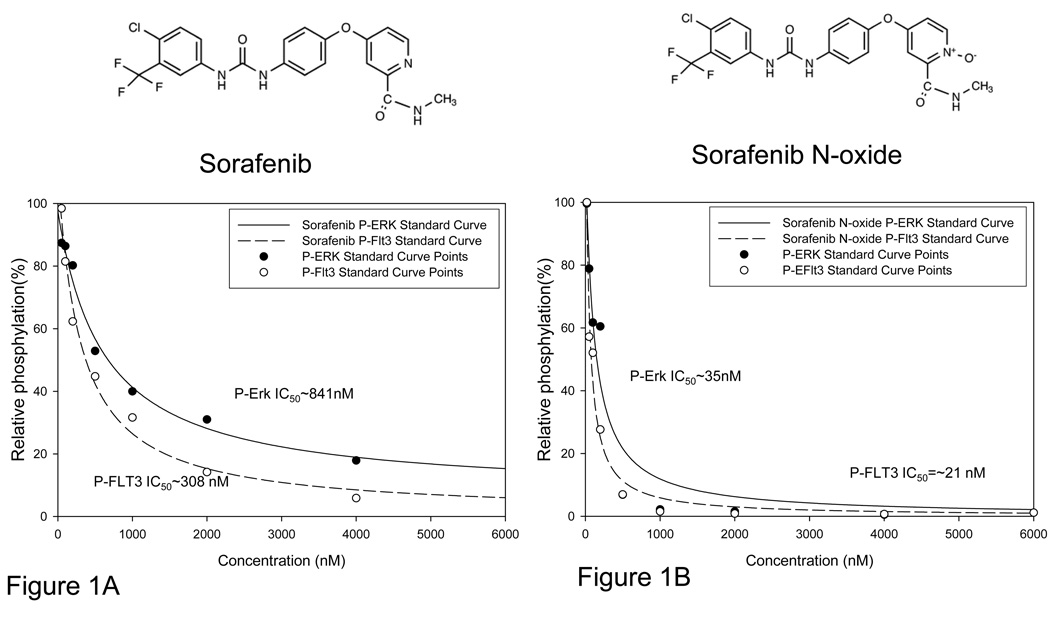
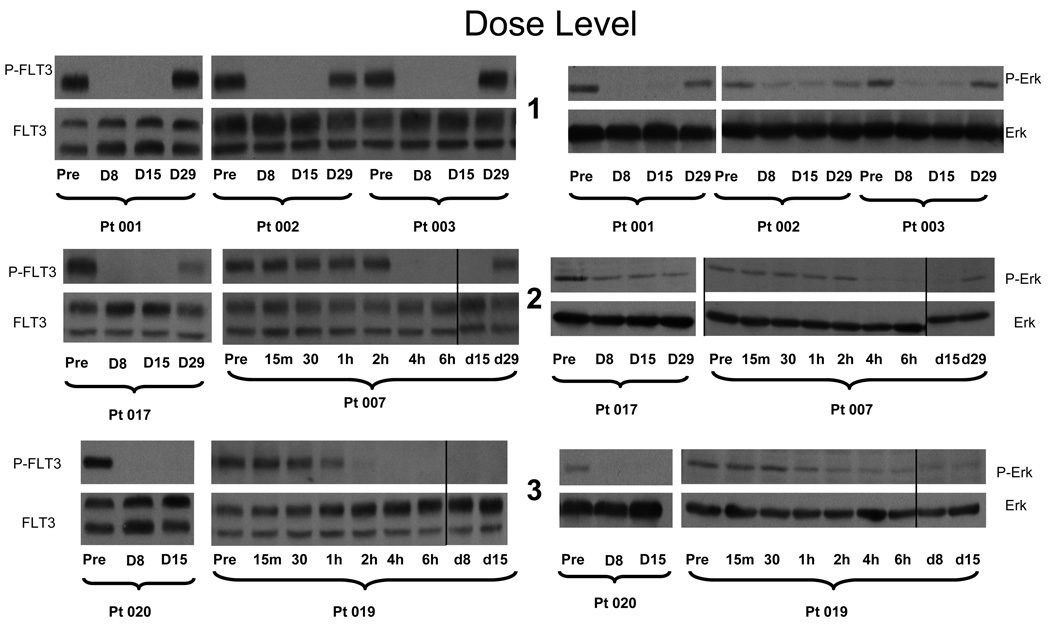
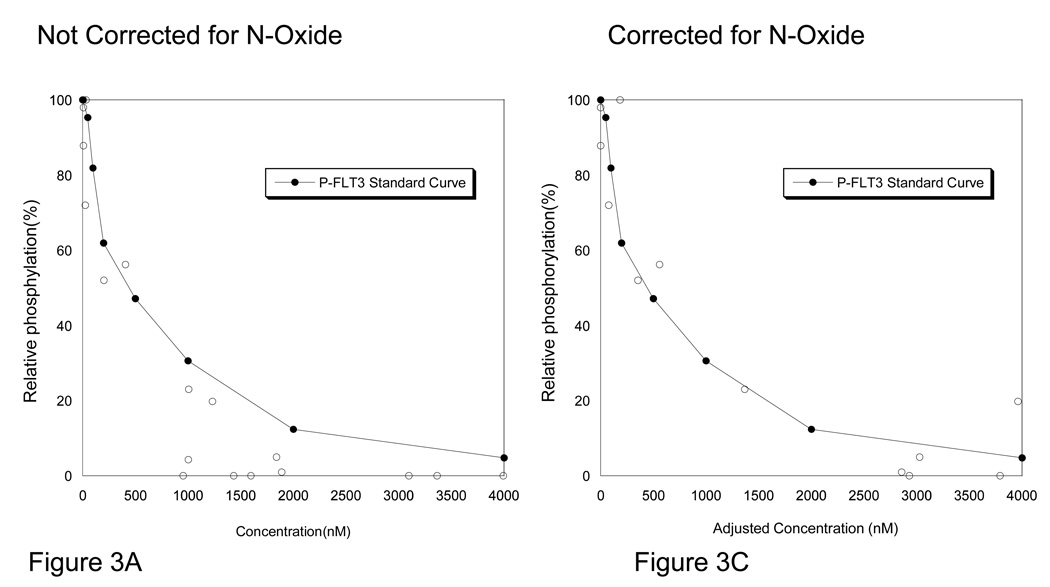
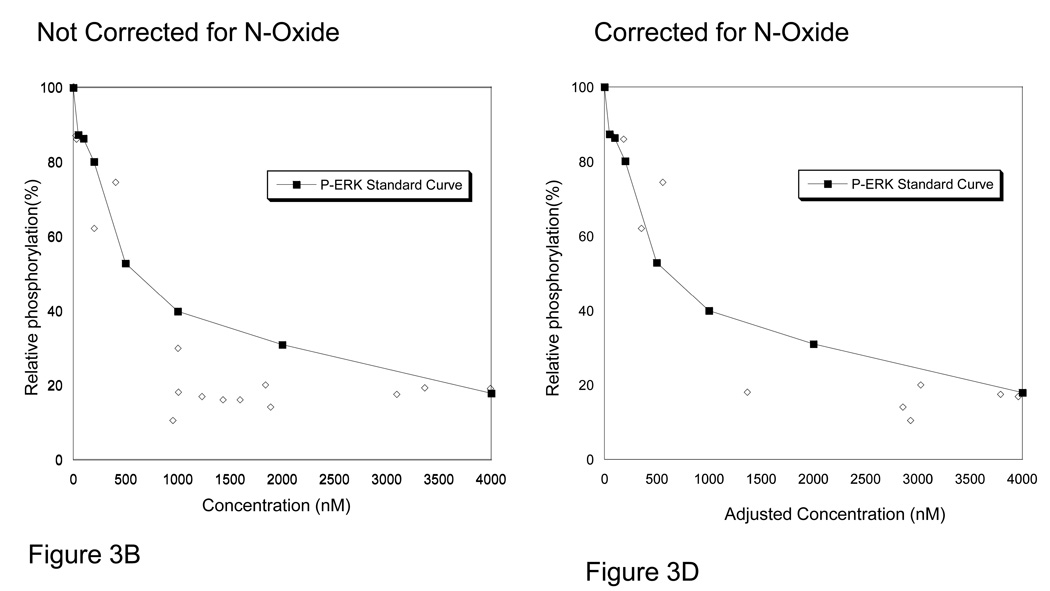
We report the results of a phase I dose escalation trial of the multikinase inhibitor sorafenib in relapsed and refractory acute leukemia patients using an intermittent dosing regimen. Fifteen patients with advanced leukemia (12 with acute myeloid leukemia, 2 with acute lymphoblastic leukemia, 1 with biphenotypic) and a median age of 63 (range 37-85) years were enrolled and treated on a dose escalation trial. Toxicities >or=grade 3 were present in 55% of cycles and the maximum tolerated dose (MTD) was determined to be 400 mg b.i.d. x 21 days in a 28-day cycle. Plasma inhibitory assays of kinase targets extracellular signal-regulated kinase (ERK) and FLT3-internal tandem duplication (ITD) showed excellent target inhibition, with FLT3-ITD silencing occurring below the MTD. The N-oxide metabolite of sorafenib seemed to be a more potent inhibitor of FLT3-ITD than the parent compound. Despite marked ex vivo FLT-3 ITD inhibition, no patients met the criteria for complete or partial response in this monotherapy study. Out of 15 patients, 11 experienced stable disease as best response. Although sorafenib showed only modest clinical activity as a single agent in this heavily treated population, robust inhibition of FLT3 and ERK suggests that there may be a potential important role in combination therapies.
Conflict of interest statement
Figures
References
-
- Larson S, Stock W. Progress in the treatment of adults with acute lymphoblastic leukemia. Curr Opin Hematol. 2008 Jul;15(4):400–407. - PubMed
-
- Tallman MS, Gilliland DG, Rowe JM. Drug therapy for acute myeloid leukemia. Blood. 2005 Aug 15;106(4):1154–1163. 2005. - PubMed
-
- Ricciardi MR, McQueen T, Chism D, Milella M, Estey E, Kaldjian E, et al. Quantitative single cell determination of ERK phosphorylation and regulation in relapsed and refractory primary acute myeloid leukemia. Leukemia. 2005 Sep;19(9):1543–1549. - PubMed
-
- Hilger RA, Scheulen ME, Strumberg D. The Ras-Raf-MEK-ERK pathway in the treatment of cancer. Onkologie. 2002 Dec;25(6):511–518. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
