Approach to urinary tract infections
- PMID: 20535247
- PMCID: PMC2875701
- DOI: 10.4103/0971-4065.59333
Approach to urinary tract infections
Abstract
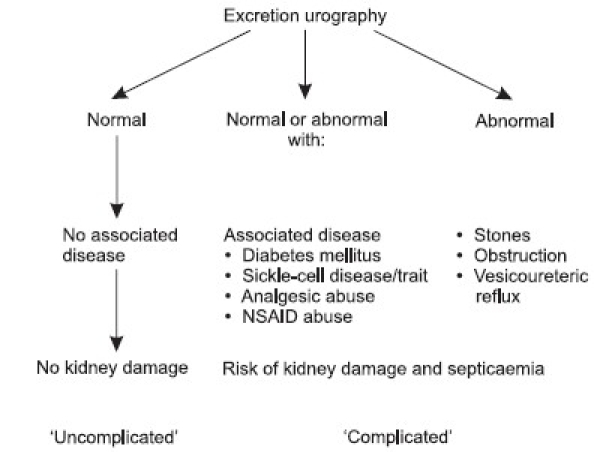
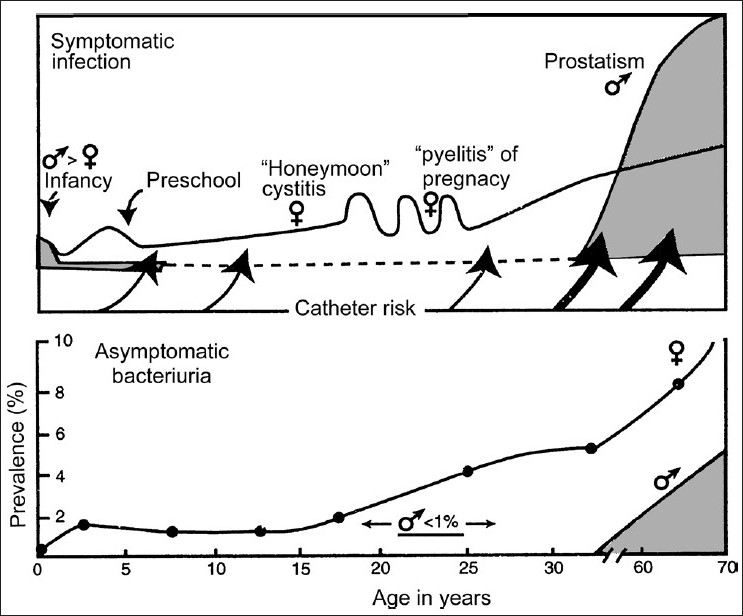
Urinary tract infection (UTI) is the most common infection experienced by humans after respiratory and gastro-intestinal infections, and also the most common cause of both community-acquired and nosocomial infections for patients admitted to hospitals. For better management and prognosis, it is mandatory to know the possible site of infection, whether the infection is uncomplicated or complicated, re-infection or relapse, or treatment failure and its pathogenesis and risk factors. Asymptomatic bacteriuria is common in certain age groups and has different connotations. It needs to be treated and completely cured in pregnant women and preschool children. Reflux nephropathy in children could result in chronic kidney disease; otherwise, urinary tract infections do not play a major role in the pathogenesis of end-stage renal disease. Symptomatic urinary tract infections occur most commonly in women of child-bearing age. Cystitis predominates, but needs to be distinguished from acute urethral syndrome that affects both sexes and has a different management plan than UTIs. The prostatitis symptoms are much more common than bacterial prostatic infections. The treatment needs to be prolonged in bacterial prostatitis and as cure rates are not very high and relapses are common, the classification of prostatitis needs to be understood. The consensus conference convened by National Institute of Health added two more groups of patients, namely, chronic prostatitis/chronic pelvic pain syndrome and asymptomatic inflammatory prostatitis, in addition to acute and chronic bacterial prostatitis. Although white blood cells in urine signify inflammation, they do not always signify UTI. Quantitative cultures of urine provide definitive evidence of UTI. Imaging studies should be done 3-6 weeks after cure of acute infection to identify abnormalities predisposing to infection or renal damage or which may affect management. Treatment of cystitis in women should be a three-day course and if symptoms are prolonged, then a seven day course of antibiotics should be given. Selected group of patients benefits from low-dose prophylactic therapy. Upper urinary tract infection may need in-patient treatment. Treatment of acute prostatitis is 30-day therapy of appropriate antibiotics and for chronic bacterial prostatitis a low dose therapy for 6-12 months may be required. It should be noted that no attempt should be made to eradicate infection unless foreign bodies such as stones and catheters are removed and correctable urological abnormalities are taken care of. Treatment under such circumstances can result only in the emergence of resistant organisms and complicate therapy further.
Keywords: Acute urethral syndrome; bacteriuria; imaging studies; low-dose prophylaxis; urinary tract infection; urine culture.
Conflict of interest statement
Figures
References
-
- Kass EH. Asymptomatic infections of the urinary tract. Trans Assoc Am Physicians. 1956;69:56–64. - PubMed
-
- Stamm WE, Counts GW, Running KR, Fihn S, Turck M, Holmes KK. Diagnosis of coliform infection in acutely dysuria women. N Engl J Med. 1982;307:463–8. - PubMed
-
- Hooton TM, Stamm WE. Diagnosis and treatment of uncomplicated urinary tract infection. Infect Dis Clin North Am. 1997;11:551–81. - PubMed
-
- Stamy TA, Govan DE, Palmer JM. The localizations and treatment of urinary tract infection: The role of bactericidal urine levels as opposed to serum levels. Medicine. 1965;44:1–36. - PubMed
-
- Baily RR. Single-dose therapy of urinary tract infection. Bolgowlah, Australia: ADIS Health Science Press; 1983.