

Patient-physician discordance in assessments of global disease severity in rheumatoid arthritis
- PMID: 20535797
- PMCID: PMC2885009
- DOI: 10.1002/acr.20132
Patient-physician discordance in assessments of global disease severity in rheumatoid arthritis
Abstract
Objective: To determine the degree of discordance between patient and physician assessment of disease severity in a multiethnic cohort of adults with rheumatoid arthritis (RA), to explore predictors of discordance, and to examine the impact of discordance on the Disease Activity Score in 28 joints (DAS28).
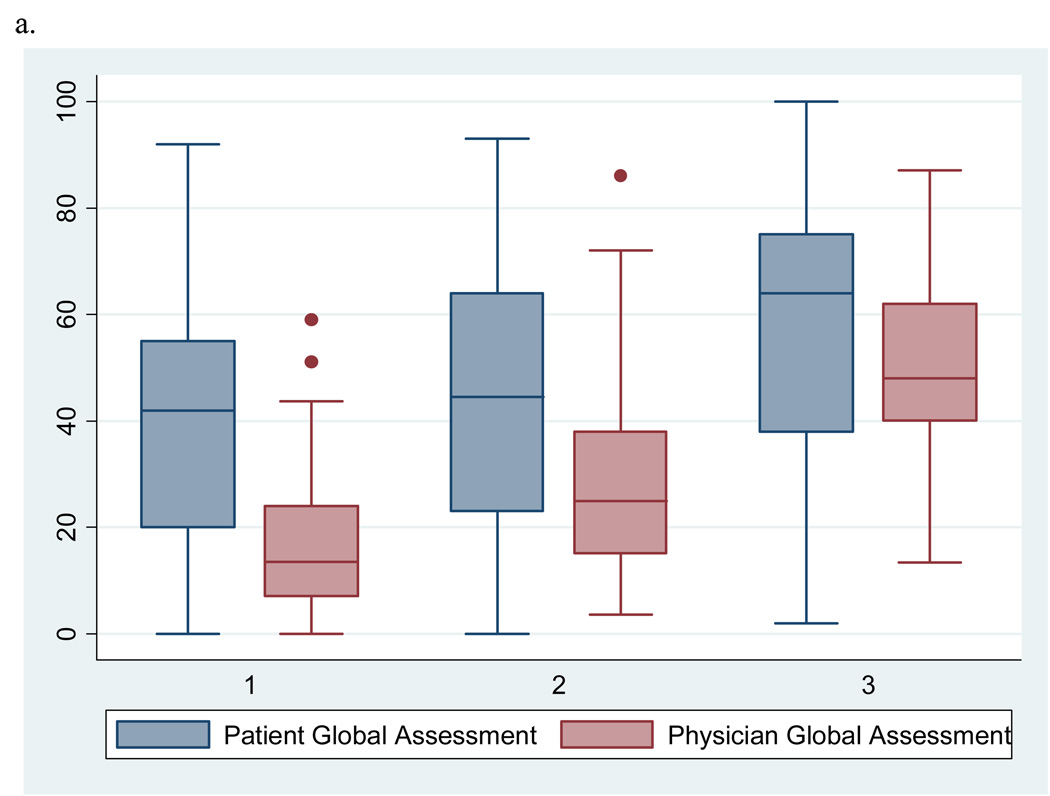
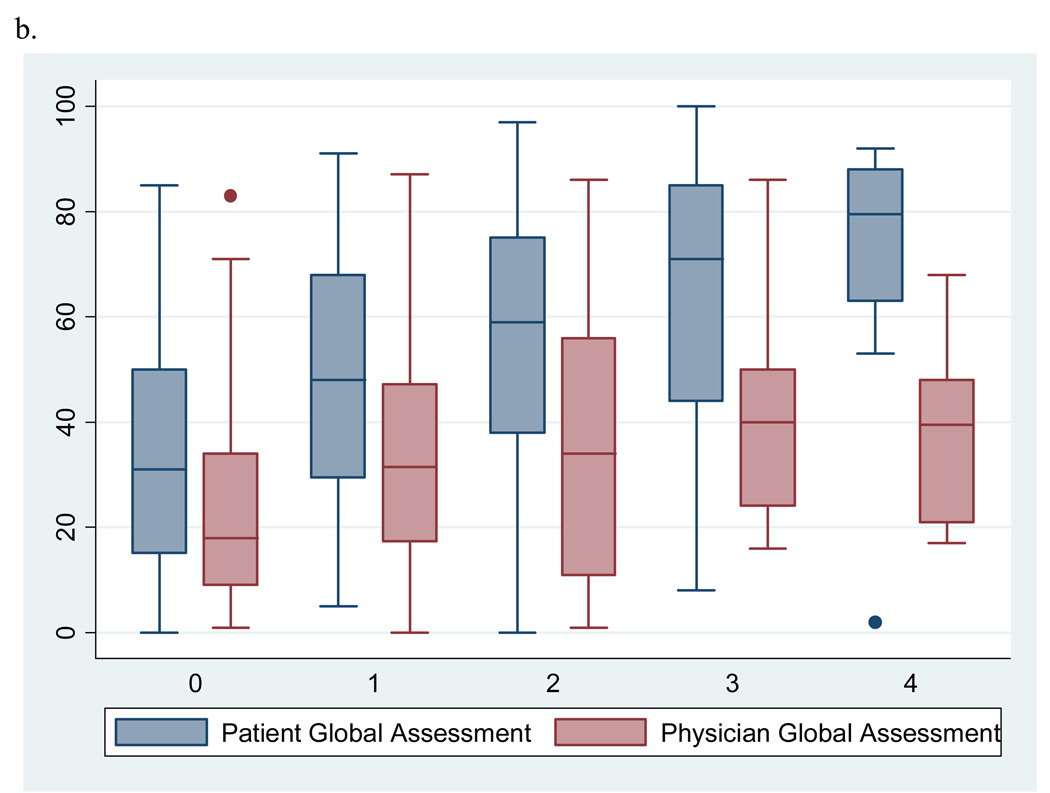
Methods: Adults with RA (n = 223) and their rheumatologists completed a visual analog scale (VAS) for global disease severity independently. Patient demographics, the 9-item Patient Health Questionnaire (PHQ-9) depression scale score, the Health Assessment Questionnaire score, and the DAS28 were also collected. Logistic regression analyses were used to identify predictors of positive discordance, defined as a patient rating minus physician rating of >25 mm on a 100-mm VAS (considered clinically relevant). DAS28 scores stratified by level of discordance were compared using a paired t-test.
Results: Positive discordance was found in 30% of cases, with a mean +/- SD difference of 46 +/- 15. The strongest independent predictor of discordance was a 5-point increase in PHQ-9 score (adjusted odds ratio 1.61, 95% confidence interval 1.02-2.55). Higher swollen joint count and Cantonese/Mandarin language were associated with lower odds of discordance. DAS28 scores were most divergent among subjects with discordance.
Conclusion: Nearly one-third of RA patients differed from their physicians to a meaningful degree in assessment of global disease severity. Higher depressive symptoms were associated with discordance. Further investigation of the relationships between mood, disease activity, and discordance may guide interventions to improve care for adults with RA.
Figures
References
-
- Prevoo ML, van 't Hof MA, Kuper HH, van Leeuwen MA, van de Putte LB, van Riel PL. Modified disease activity scores that include twenty-eight-joint counts. Development and validation in a prospective longitudinal study of patients with rheumatoid arthritis. Arthritis Rheum. 1995;38(1):44–48. - PubMed
-
- Saag KG, Teng GG, Patkar NM, Anuntiyo J, Finney C, Curtis JR, et al. American College of Rheumatology 2008 recommendations for the use of nonbiologic and biologic disease-modifying antirheumatic drugs in rheumatoid arthritis. Arthritis Rheum. 2008;59(6):762–784. - PubMed
-
- Neville C, Clarke AE, Joseph L, Belisle P, Ferland D, Fortin PR. Learning from discordance in patient and physician global assessments of systemic lupus erythematosus disease activity. J Rheumatol. 2000;27(3):675–679. - PubMed
-
- Felson DT, Anderson JJ, Boers M, Bombardier C, Chernoff M, Fried B, et al. The Committee on Outcome Measures in Rheumatoid Arthritis Clinical Trials. The American College of Rheumatology preliminary core set of disease activity measures for rheumatoid arthritis clinical trials. Arthritis Rheum. 1993;36(6):729–740. - PubMed
-
- Nicolau G, Yogui MM, Vallochi TL, Gianini RJ, Laurindo IM, Novaes GS. Sources of discrepancy in patient and physician global assessments of rheumatoid arthritis disease activity. J Rheumatol. 2004;31(7):1293–1296. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
