

Weekly self-monitoring and treatment adjustment benefit patients with partly controlled and uncontrolled asthma: an analysis of the SMASHING study
- PMID: 20537124
- PMCID: PMC2893513
- DOI: 10.1186/1465-9921-11-74
Weekly self-monitoring and treatment adjustment benefit patients with partly controlled and uncontrolled asthma: an analysis of the SMASHING study
Abstract
Background: Internet-based self-management has shown to improve asthma control and asthma related quality of life, but the improvements were only marginally clinically relevant for the group as a whole. We hypothesized that self-management guided by weekly monitoring of asthma control tailors pharmacological therapy to individual needs and improves asthma control for patients with partly controlled or uncontrolled asthma.
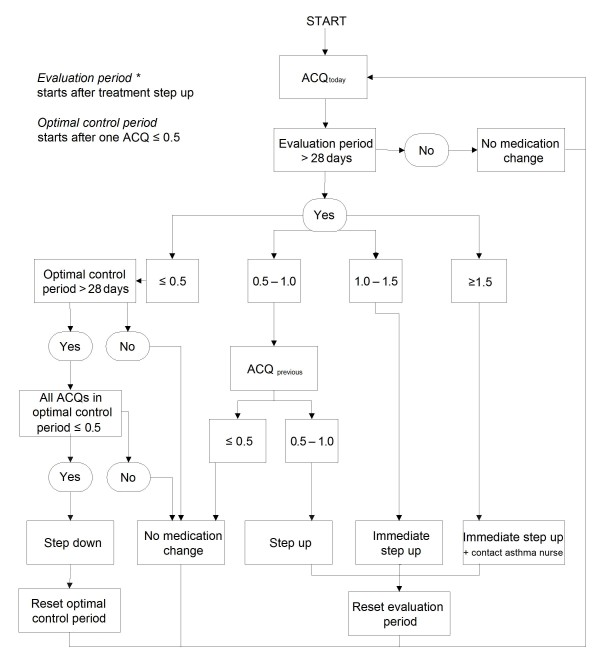
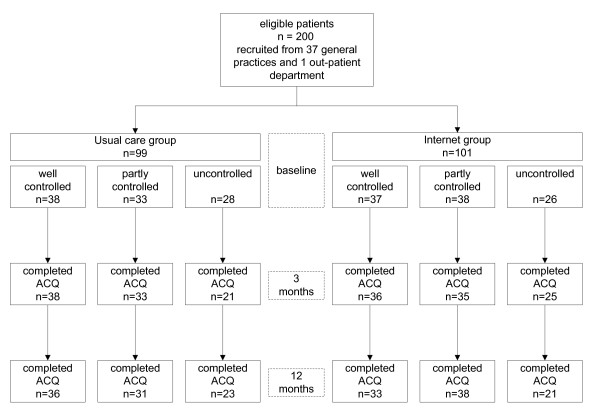
Methods: In a 1-year randomised controlled trial involving 200 adults (18-50 years) with mild to moderate persistent asthma we evaluated the adherence with weekly monitoring and effect on asthma control and pharmacological treatment of a self-management algorithm based on the Asthma Control Questionnaire (ACQ). Participants were assigned either to the Internet group (n = 101) that monitored asthma control weekly with the ACQ on the Internet and adjusted treatment using a self-management algorithm supervised by an asthma nurse specialist or to the usual care group (UC) (n = 99). We analysed 3 subgroups: patients with well controlled (ACQ <or= 0.75), partly controlled (0.75>ACQ <or= 1.5) or uncontrolled (ACQ>1.5) asthma at baseline.
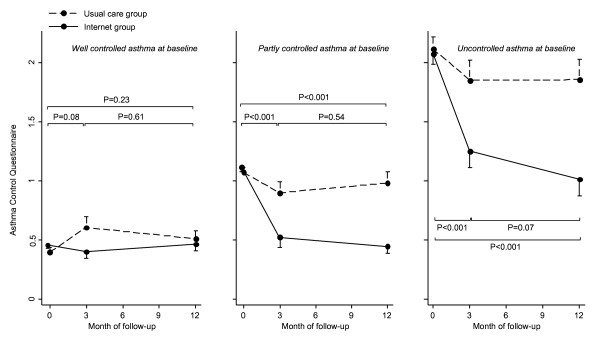
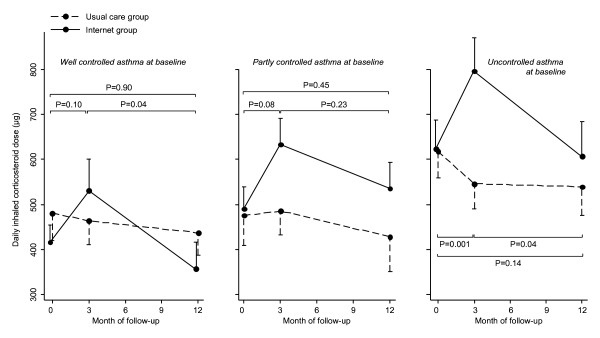
Results: Overall monitoring adherence was 67% (95% CI, 60% to 74%). Improvements in ACQ score after 12 months were -0.14 (p = 0.23), -0.52 (p < 0.001) and -0.82 (p < 0.001) in the Internet group compared to usual care for patients with well, partly and uncontrolled asthma at baseline, respectively. Daily inhaled corticosteroid dose significantly increased in the Internet group compared to usual care in the first 3 months in patients with uncontrolled asthma (+278 microg, p = 0.001), but not in patients with well or partly controlled asthma. After one year there were no differences in daily inhaled corticosteroid use or long-acting beta2-agonists between the Internet group and usual care.
Conclusions: Weekly self-monitoring and subsequent treatment adjustment leads to improved asthma control in patients with partly and uncontrolled asthma at baseline and tailors asthma medication to individual patients' needs.
Figures

References
-
- National Heart Lung and Blood Institute. National Asthma Education and Prevention Program(NAEPP) Expert panel report 3: Guidelines for the Diagnosis and Management of Asthma. 2007.
-
- Taylor DR, Bateman ED, Boulet L-P, Boushey HA, Busse WW, Casale TB, Chanez P, Enright PL, Gibson PG, de Jongste JC, Kerstjens HA, Lazarus SC, Levy ML, O'Byrne PM, Partridge MR, Pavord ID, Sears MR, Sterk PJ, Stoloff SW, Szefler SJ, Sullivan SD, Thomas MD, Wenzel SE, Reddel HK. A new perspective on concepts of asthma severity and control. Eur Respir J. 2008;32:545–554. doi: 10.1183/09031936.00155307. - DOI - PubMed
-
- National Institutes of Health. Global initiative for asthma. Global strategy for asthma management and prevention. NIH Publication No 02-3659; Issued January 1995 (Updated 2006)
-
- Vollmer WM, Markson LE, O'Connor E, Frazier EA, Berger M, Buist AS. Association of asthma control with health care utilization and quality of life. Am J Respir Crit Care Med. 1999;160:1647–652. - PubMed
