

Congenital hypothyroidism
- PMID: 20537182
- PMCID: PMC2903524
- DOI: 10.1186/1750-1172-5-17
Congenital hypothyroidism
Abstract
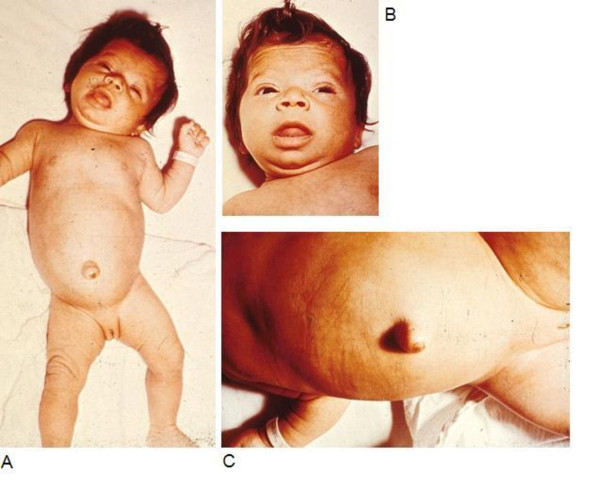
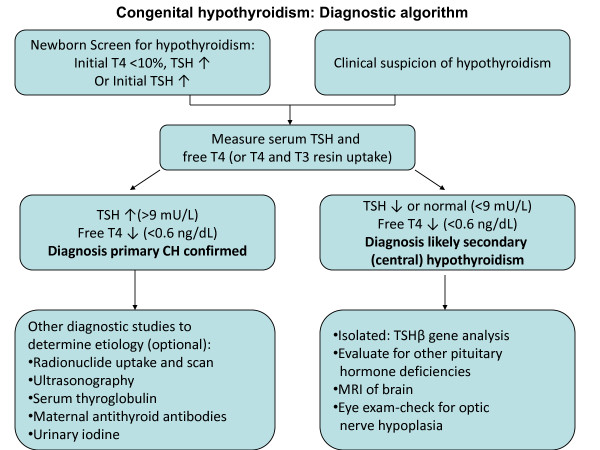
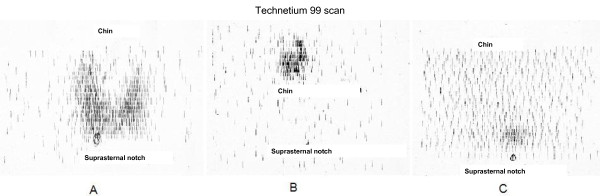
Congenital hypothyroidism (CH) occurs in approximately 1:2,000 to 1:4,000 newborns. The clinical manifestations are often subtle or not present at birth. This likely is due to trans-placental passage of some maternal thyroid hormone, while many infants have some thyroid production of their own. Common symptoms include decreased activity and increased sleep, feeding difficulty, constipation, and prolonged jaundice. On examination, common signs include myxedematous facies, large fontanels, macroglossia, a distended abdomen with umbilical hernia, and hypotonia. CH is classified into permanent and transient forms, which in turn can be divided into primary, secondary, or peripheral etiologies. Thyroid dysgenesis accounts for 85% of permanent, primary CH, while inborn errors of thyroid hormone biosynthesis (dyshormonogeneses) account for 10-15% of cases. Secondary or central CH may occur with isolated TSH deficiency, but more commonly it is associated with congenital hypopitiutarism. Transient CH most commonly occurs in preterm infants born in areas of endemic iodine deficiency. In countries with newborn screening programs in place, infants with CH are diagnosed after detection by screening tests. The diagnosis should be confirmed by finding an elevated serum TSH and low T4 or free T4 level. Other diagnostic tests, such as thyroid radionuclide uptake and scan, thyroid sonography, or serum thyroglobulin determination may help pinpoint the underlying etiology, although treatment may be started without these tests. Levothyroxine is the treatment of choice; the recommended starting dose is 10 to 15 mcg/kg/day. The immediate goals of treatment are to rapidly raise the serum T4 above 130 nmol/L (10 ug/dL) and normalize serum TSH levels. Frequent laboratory monitoring in infancy is essential to ensure optimal neurocognitive outcome. Serum TSH and free T4 should be measured every 1-2 months in the first 6 months of life and every 3-4 months thereafter. In general, the prognosis of infants detected by screening and started on treatment early is excellent, with IQs similar to sibling or classmate controls. Studies show that a lower neurocognitive outcome may occur in those infants started at a later age (> 30 days of age), on lower l-thyroxine doses than currently recommended, and in those infants with more severe hypothyroidism.
Figures


References
-
- Gaudino R, Garel C, Czernichow P, Leger J. Proportion of various types of thyroid disorders among newborns with congenital hypothyroidism and normally located gland: a regional cohort study. ClinEndocrinol(Oxf) 2005;62(4):444–448. - PubMed
-
- Skordis N, Toumba M, Savva SC, Erakleous E, Topouzi M, Vogazianos M, Argyriou A. High prevalence of congenital hypothyroidism in the Greek Cypriot population: results of the neonatal screening program 1990-2000. JPediatrEndocrinol. 2005;18(5):453–461. - PubMed
-
- Harris KB, Pass KA. Increase in congenital hypothyroidism in New York State and in the United States. MolGenetMetab. 2007;91(3):268–277. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
