

Continuous versus bolus dosing of Furosemide for patients hospitalized for heart failure
- PMID: 20538132
- PMCID: PMC3900281
- DOI: 10.1016/j.amjcard.2010.01.355
Continuous versus bolus dosing of Furosemide for patients hospitalized for heart failure
Abstract
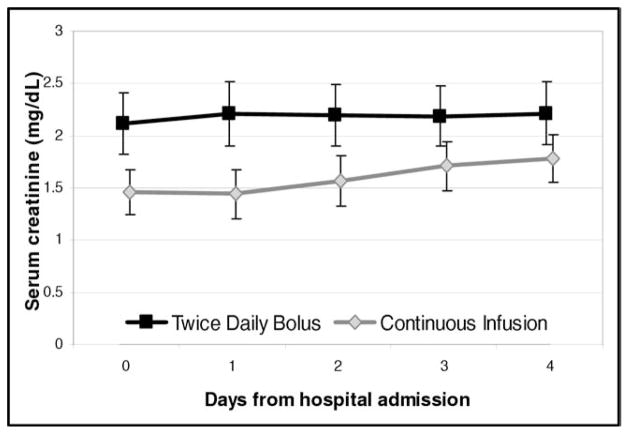
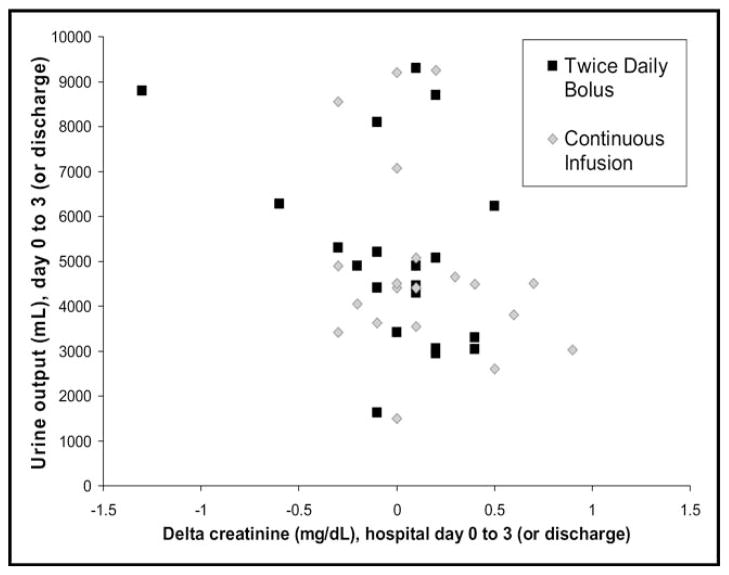
Intravenous diuretics are the cornerstone of management for patients hospitalized for heart failure. Physiologic data suggest that intermittent high-dose furosemide promotes neurohormonal activation, which a slow continuous infusion might remediate. However, the limited clinical data comparing dosing schemes are confounded. This study was a randomized, open-label, single-center trial of twice-daily bolus injection versus continuous infusion furosemide in patients hospitalized with heart failure and volume overload. The primary outcome was change in creatinine from admission to hospital day 3 or discharge. Twenty-one patients were randomized to bolus injection and 20 patients to continuous infusion. Baseline characteristics were balanced between study arms except for gender, with a mean age of 60 +/- 15 years, a mean ejection fraction of 35 +/- 19%, and a mean creatinine level of 1.9 +/- 1.2 mg/dl. The mean doses of furosemide were similar between arms over the first 48 hours (162 +/- 48 and 162 +/- 52 mg/24 hours). None of the outcomes differed significantly between bolus and continuous dosing from admission to hospital day 3 or discharge (mean change in creatinine -0.02 vs 0.13 mg/dl, p = 0.18; urine output 5,113 vs 4,894 ml, p = 0.78; length of stay 8.8 vs 9.9 days, p = 0.69). All patients survived to discharge. In conclusion, there were no substantial differences between bolus injection and continuous infusion of equal doses of furosemide for the treatment of patients hospitalized with heart failure. Given the high prevalence of heart failure hospitalization and the disparate results of small studies regarding optimal dosing of loop diuretics to treat these patients, larger multicenter blinded studies are needed.
Figures
References
-
- Adams KF, Jr, Fonarow GC, Emerman CL, LeJemtel TH, Costanzo MR, Abraham WT, Berkowitz RL, Galvao M, Horton DP. Characteristics and outcomes of patients hospitalized for heart failure in the United States: rationale, design, and preliminary observations from the first 100,000 cases in the Acute Decompensated Heart Failure National Registry (ADHERE) Am Heart J. 2005;149:209–216. - PubMed
-
- Shah MR, Stevenson LW. Searching for evidence: refractory questions in advanced heart failure. J Card Fail. 2004;10:210–218. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
