

Feasibility of intra-arrest hypothermia induction: A novel nasopharyngeal approach achieves preferential brain cooling
- PMID: 20538402
- PMCID: PMC4565604
- DOI: 10.1016/j.resuscitation.2010.04.005
Feasibility of intra-arrest hypothermia induction: A novel nasopharyngeal approach achieves preferential brain cooling
Abstract
Aim: In patients with cardiopulmonary arrest, brain cooling may improve neurological outcome, especially if applied prior to or during early reperfusion. Thus it is important to develop feasible cooling methods for pre-hospital use. This study examines cerebral and compartmental thermokinetic properties of nasopharyngeal cooling during various blood flow states.
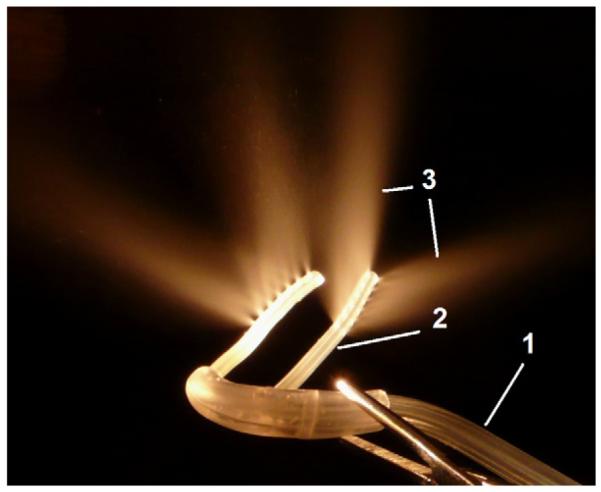
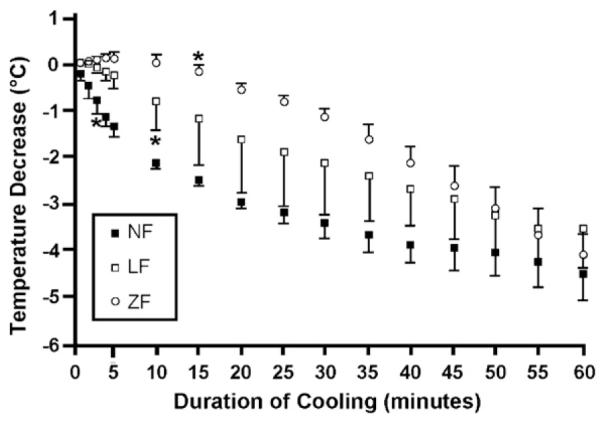
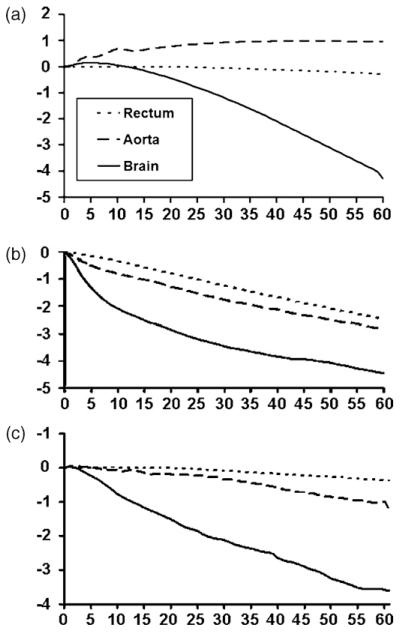
Methods: Ten swine (40+/-4kg) were anesthetized, intubated and monitored. Temperature was determined in the frontal lobe of the brain, in the aorta, and in the rectum. After the preparatory phase the cooling device (RhinoChill system), which produces evaporative cooling in the nasopharyngeal area, was activated for 60min. The thermokinetic response was evaluated during stable anaesthesia (NF, n=3); during untreated cardiopulmonary arrest (ZF, n=3); during CPR (LF, n=4).
Results: Effective brain cooling was achieved in all groups with a median cerebral temperature decrease of -4.7 degrees C for NF, -4.3 degrees C for ZF and -3.4 degrees C for LF after 60min. The initial brain cooling rate however was fastest in NF, followed by LF, and was slowest in ZF; the median brain temperature decrease from baseline after 15min of cooling was -2.48 degrees C for NF, -0.12 degrees C for ZF, and -0.93 degrees C for LF, respectively. A median aortic temperature change of -2.76 degrees C for NF, -0.97 for LF and +1.1 degrees C for ZF after 60min indicated preferential brain cooling in all groups.
Conclusion: While nasopharyngeal cooling in swine is effective at producing preferential cerebral hypothermia in various blood flow states, initial brain cooling is most efficient with normal circulation.
Copyright 2010 Elsevier Ireland Ltd. All rights reserved.
Figures
Similar articles
-
Safety and feasibility of nasopharyngeal evaporative cooling in the emergency department setting in survivors of cardiac arrest.Resuscitation. 2010 Aug;81(8):943-9. doi: 10.1016/j.resuscitation.2010.04.027. Epub 2010 Jun 2. Resuscitation. 2010. PMID: 20627524 Clinical Trial.
-
Intra-arrest selective brain cooling improves success of resuscitation in a porcine model of prolonged cardiac arrest.Resuscitation. 2010 May;81(5):617-21. doi: 10.1016/j.resuscitation.2010.01.027. Epub 2010 Mar 6. Resuscitation. 2010. PMID: 20207471
-
Selective brain cooling in infant piglets after cardiac arrest and resuscitation.Crit Care Med. 1996 Jun;24(6):1009-17. doi: 10.1097/00003246-199606000-00022. Crit Care Med. 1996. PMID: 8681567
-
Mild hypothermia and outcome after CPR. Hypothermia for Cardiac Arrest (HACA) Study Group.Acta Anaesthesiol Scand Suppl. 1997;111:55-8. Acta Anaesthesiol Scand Suppl. 1997. PMID: 9420956 Review. No abstract available.
-
Is hypothermia indicated during cardiopulmonary resuscitation and after restoration of spontaneous circulation?Curr Opin Crit Care. 2016 Jun;22(3):212-7. doi: 10.1097/MCC.0000000000000299. Curr Opin Crit Care. 2016. PMID: 27029051 Review.
Cited by
-
A new approach to selective brain cooling by a Ranque-Hilsch vortex tube.Intensive Care Med Exp. 2016 Dec;4(1):32. doi: 10.1186/s40635-016-0102-5. Epub 2016 Sep 29. Intensive Care Med Exp. 2016. PMID: 27686339 Free PMC article.
-
From systemic to selective brain cooling - Methods in review.Brain Circ. 2019 Dec 27;5(4):179-186. doi: 10.4103/bc.bc_23_19. eCollection 2019 Oct-Dec. Brain Circ. 2019. PMID: 31950093 Free PMC article. Review.
-
Inducing Brain Cooling Without Core Temperature Reduction in Pigs Using a Novel Nasopharyngeal Method: An Effectiveness and Safety Study.Neurocrit Care. 2020 Apr;32(2):564-574. doi: 10.1007/s12028-019-00789-2. Neurocrit Care. 2020. PMID: 31317319 Free PMC article.
-
Selection of preclinical models to evaluate intranasal brain cooling for acute ischemic stroke.Brain Circ. 2019 Dec 27;5(4):160-168. doi: 10.4103/bc.bc_20_19. eCollection 2019 Oct-Dec. Brain Circ. 2019. PMID: 31950091 Free PMC article. Review.
-
Updates on Selective Brain Hypothermia: Studies From Bench Work to Clinical Trials.Front Neurol. 2022 May 6;13:899547. doi: 10.3389/fneur.2022.899547. eCollection 2022. Front Neurol. 2022. PMID: 35599727 Free PMC article. Review.
References
-
- Nichol G, Rumsfeld J, Eigel B, et al. Essential features of designating outof-hospital cardiac arrest as a reportable event: a scientific statement from the American Heart Association Emergency Cardiovascular Care Committee; Council on Cardiopulmonary, Perioperative, and Critical Care; Council on Cardiovascular Nursing; Council on Clinical Cardiology; and Quality of Care and Outcomes Research Interdisciplinary Working Group. Circulation. 2008;117:2299–308. - PubMed
-
- Geocadin RG, Koenig MA, Stevens RD, et al. Intensive care for brain injury after cardiac arrest: therapeutic hypothermia and related neuroprotective strategies. Crit Care Clin. 2006;22:619, 36. abstract viii. - PubMed
-
- Neumar RW, Nolan JP, Adrie C, et al. Post-cardiac arrest syndrome: epidemiology, pathophysiology, treatment, and prognostication. A consensus statement from the International Liaison Committee on Resuscitation (American Heart Association, Australian and New Zealand Council on Resuscitation, European Resuscitation Council, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Council of Asia, and the Resuscitation Council of Southern Africa); the American Heart Association Emergency Cardiovascular Care Committee; the Council on Cardiovascular Surgery and Anesthesia; the Council on Cardiopulmonary, Perioperative, and Critical Care; the Council on Clinical Cardiology; and the Stroke Council. Circulation. 2008;118:2452–83. - PubMed
-
- Leonov Y, Sterz F, Safar P, et al. Mild cerebral hypothermia during and after cardiac arrest improves neurologic outcome in dogs. J Cereb Blood Flow Metab. 1990;10:57–70. - PubMed
-
- Bernard SA, Gray TW, Buist MD, et al. Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. N Engl J Med. 2002;346:557–63. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
