

Cost-effectiveness of CT perfusion for selecting patients for intravenous thrombolysis: a US hospital perspective
- PMID: 20538823
- PMCID: PMC7965001
- DOI: 10.3174/ajnr.A2138
Cost-effectiveness of CT perfusion for selecting patients for intravenous thrombolysis: a US hospital perspective
Abstract
Background and purpose: Improved selection of patients with stroke for IV tPA treatment may enhance clinical outcomes. Given the limited availability of MR imaging in hospitals, we examined the cost-effectiveness of adding CTP to the usual CT-based methods for selecting patients on the basis of the presence and extent of penumbra.
Materials and methods: A decision-analytic model estimated the costs and outcomes associated with penumbra-based CTP selection in a patient population similar to that enrolled in the IV tPA clinical trials. Model inputs were obtained from published literature, clinical trial data, standard US costing sources, and expert opinion. Cost per life-year saved and cost per QALY gained were estimated from a hospital perspective.
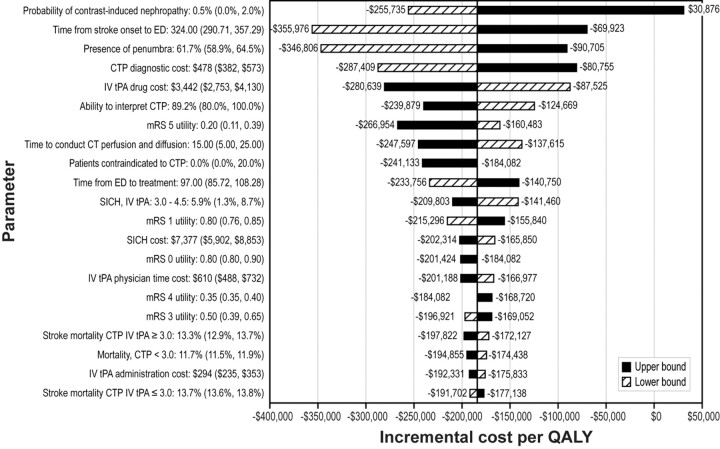
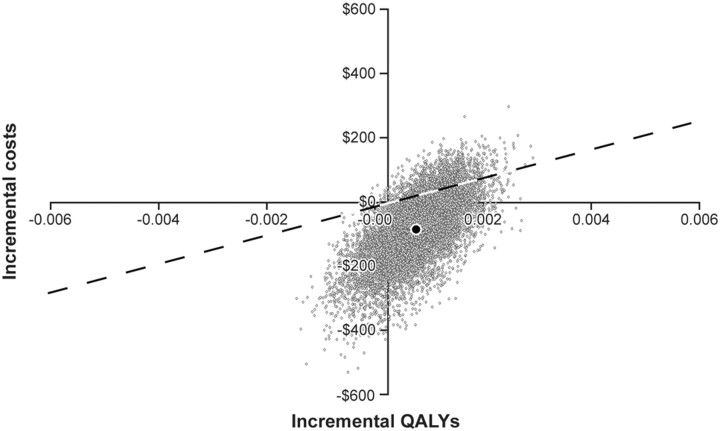
Results: Addition of penumbra-based CTP to standard unenhanced CT improved favorable outcome (mRS, ≤1) by 0.59% and reduced cost by $42 compared with selection based on unenhanced CT alone. Life-years and QALYs improved. Multivariate sensitivity analysis predicted cost-effectiveness (≤$50,000 per QALY) in 89.2% of simulation runs.
Conclusions: Using penumbra-based CTP after routine CT to select patients with ischemic stroke for IV tPA is cost-effective compared with the usual CT-based methods for hospitals. With the ease of access of CTP, penumbra-based selection methods may be readily available to hospitals. Thus, this economic analysis may lend further support to the consideration of a paradigm shift in acute stroke evaluation.
Figures
References
-
- Adams HP, Jr, del Zoppo G, Alberts MJ, et al. , for the American Heart Association, American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups. Guidelines for the early management of adults with ischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups—the American Academy of Neurology affirms the value of this guideline as an educational tool for neurologists. Stroke 2007; 38: 1655– 711 - PubMed
-
- Intercollegiate Stroke Working Party. National Clinical Guidelines for Stroke. London: Royal College of Physicians; 2004
-
- Thomalla G, Schwark C, Sobesky J, et al. . Outcome and symptomatic bleeding complications of intravenous thrombolysis within 6 hours in MRI-selected stroke patients: comparison of a German multicenter study with the pooled data of ATLANTIS, ECASS, and NINDS tPA trials. Stroke 2006; 37: 852– 58 - PubMed
-
- Schellinger PD, Thomalla G, Fiehler J, et al. . MRI-based and CT-based thrombolytic therapy in acute stroke within and beyond established time windows: an analysis of 1210 patients. Stroke 2007; 38: 2640– 45 - PubMed
-
- Wintermark M, Flanders AE, Velthuis B, et al. . Perfusion-CT assessment of infarct core and penumbra receiver operating characteristic curve analysis in 130 patients suspected of acute hemispheric stroke. Stroke 2006; 37: 979– 85 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical